Hand and wrist arthritis describes the loss of joint cartilage and the inflammatory or mechanical changes that follow. The three most common forms are osteoarthritis (the wear-and-tear pattern affecting the DIP, PIP, thumb CMC, and wrist), rheumatoid arthritis (an autoimmune disease that destroys joint cartilage and bone), and post-traumatic arthritis (the long-term consequence of an old fracture or ligament injury). Treatment ranges from anti-inflammatory medication, splinting, and corticosteroid injection to joint replacement (arthroplasty) or fusion (arthrodesis) for end-stage disease.
The Anatomy of a Joint
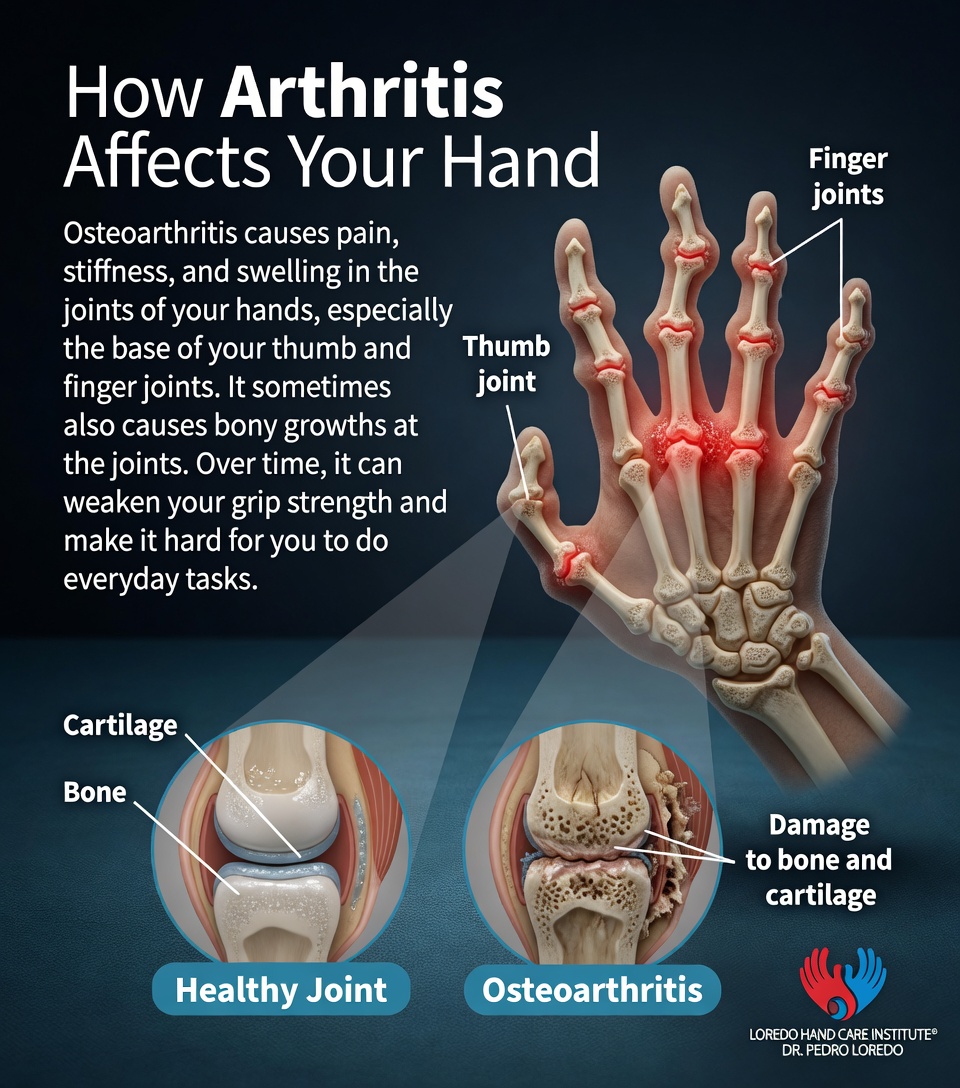
Cartilage caps the ends of every bone in a joint, providing a smooth gliding surface and cushioning load. The synovial membrane lines the joint and produces fluid that lubricates motion. In osteoarthritis, cartilage gradually wears away, the joint space narrows, bone rubs on bone, and osteophytes (bone spurs) form at the margins. In rheumatoid arthritis, an autoimmune attack on the synovial lining drives cartilage and bone destruction, often symmetrically and at multiple joints. In post-traumatic arthritis, an old fracture or ligament injury alters joint mechanics and accelerates cartilage wear at that specific joint.
The most commonly affected joints in the hand are the distal interphalangeal (DIP) joints, the proximal interphalangeal (PIP) joints, the thumb carpometacarpal (CMC) joint, and the wrist. The metacarpophalangeal (MCP) joints are most often involved in rheumatoid arthritis.
Clinical coding: ICD-10 M19.0 (primary osteoarthritis, multiple sites). M06.9 (rheumatoid arthritis, unspecified). SNOMED CT 396275006 (osteoarthritis), 69896004 (rheumatoid arthritis).
Causes and Risk Factors
- Age: osteoarthritis risk rises steadily after 50
- Female sex, particularly for DIP, PIP, and thumb CMC osteoarthritis
- Family history, with a clear genetic component for both OA and RA
- Prior trauma: fracture or significant ligament injury at the joint
- Prior infection in the joint (septic arthritis)
- Autoimmune disease: rheumatoid, psoriatic, lupus, gout
- Repetitive heavy use in manual occupations
- Smoking, which is a clear risk factor for rheumatoid arthritis severity
Symptoms and Warning Signs
- Joint pain, often deep and aching, worse with use and at the end of the day
- Morning stiffness (in RA classically more than 1 hour, in OA less than 30 minutes)
- Joint swelling and warmth, more prominent in inflammatory arthritis
- Loss of grip strength and difficulty with fine pinch
- Visible nodules at fingertip joints (Heberden's) or middle finger joints (Bouchard's)
- Joint deformity, including ulnar deviation of the fingers in advanced rheumatoid disease
- Crepitus, a grinding sensation with motion
- Loss of motion at the affected joint
Understanding Finger Arthritis Progression
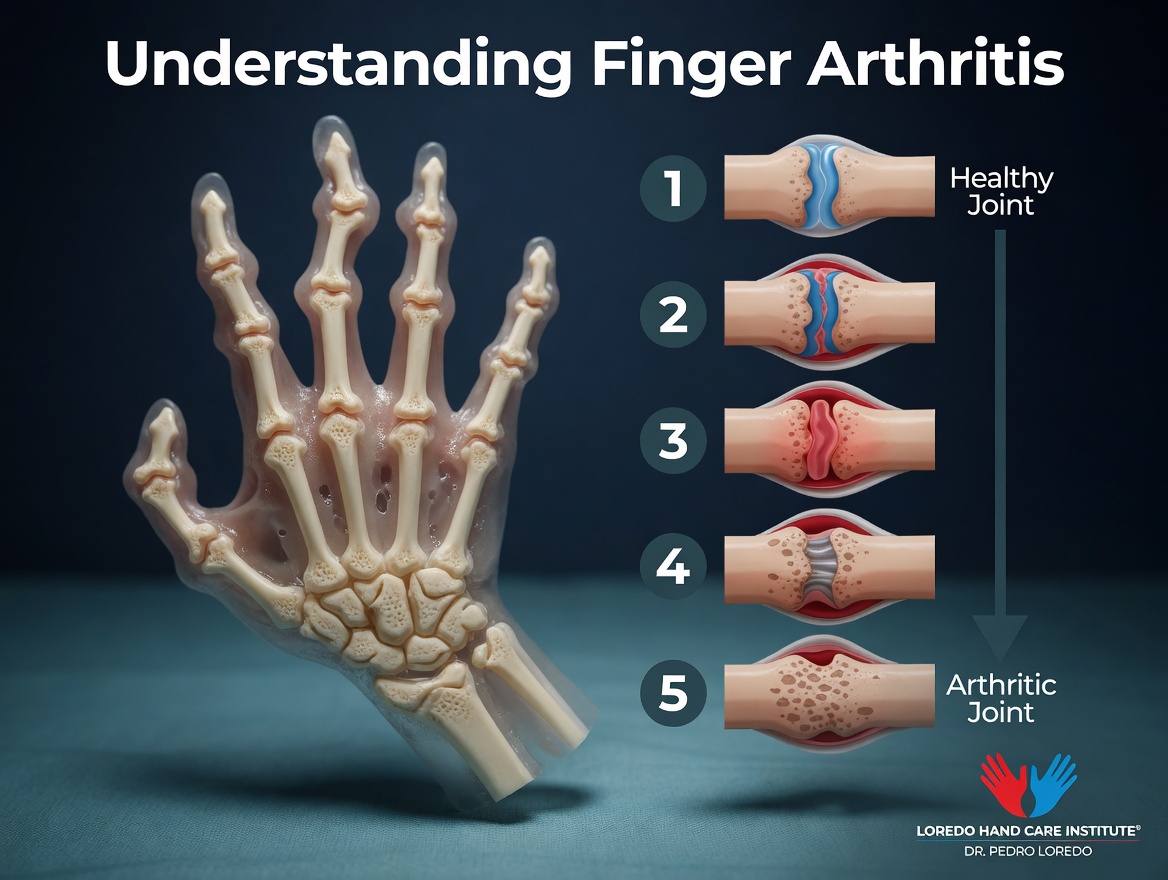
Finger arthritis develops gradually. Stage 1 shows a healthy joint with intact cartilage and full motion. Stage 2 begins with mild cartilage thinning, often without symptoms. Stage 3 brings noticeable joint space narrowing and the first symptoms of pain and stiffness. Stage 4 shows substantial cartilage loss with bone changes including osteophytes (bone spurs). Stage 5 is the end-stage arthritic joint with bone-on-bone contact, severe pain, and visible deformity. Treatment options expand at every stage, with conservative care effective in early stages and surgical reconstruction reserved for advanced disease.
How OA, RA, and Post-Traumatic Arthritis Differ
- Onset: OA is gradual and age-related. RA can appear at any age, often in the 30s to 50s. Post-traumatic arthritis is linked to a specific past injury.
- Pattern: OA is asymmetric and concentrates at DIP, PIP, thumb CMC, and wrist. RA is symmetric and concentrates at MCP, wrist, and PIP joints. Post-traumatic arthritis affects only the joint that was injured.
- Morning stiffness: less than 30 minutes in OA, more than 1 hour in RA, variable after trauma.
- Lab tests: normal in OA. RA shows positive rheumatoid factor, anti-CCP antibodies, and elevated inflammatory markers (ESR, CRP).
- X-ray pattern: joint space narrowing and osteophytes in OA. Erosions and periarticular osteopenia in RA. Old fracture lines and joint incongruity in post-traumatic.
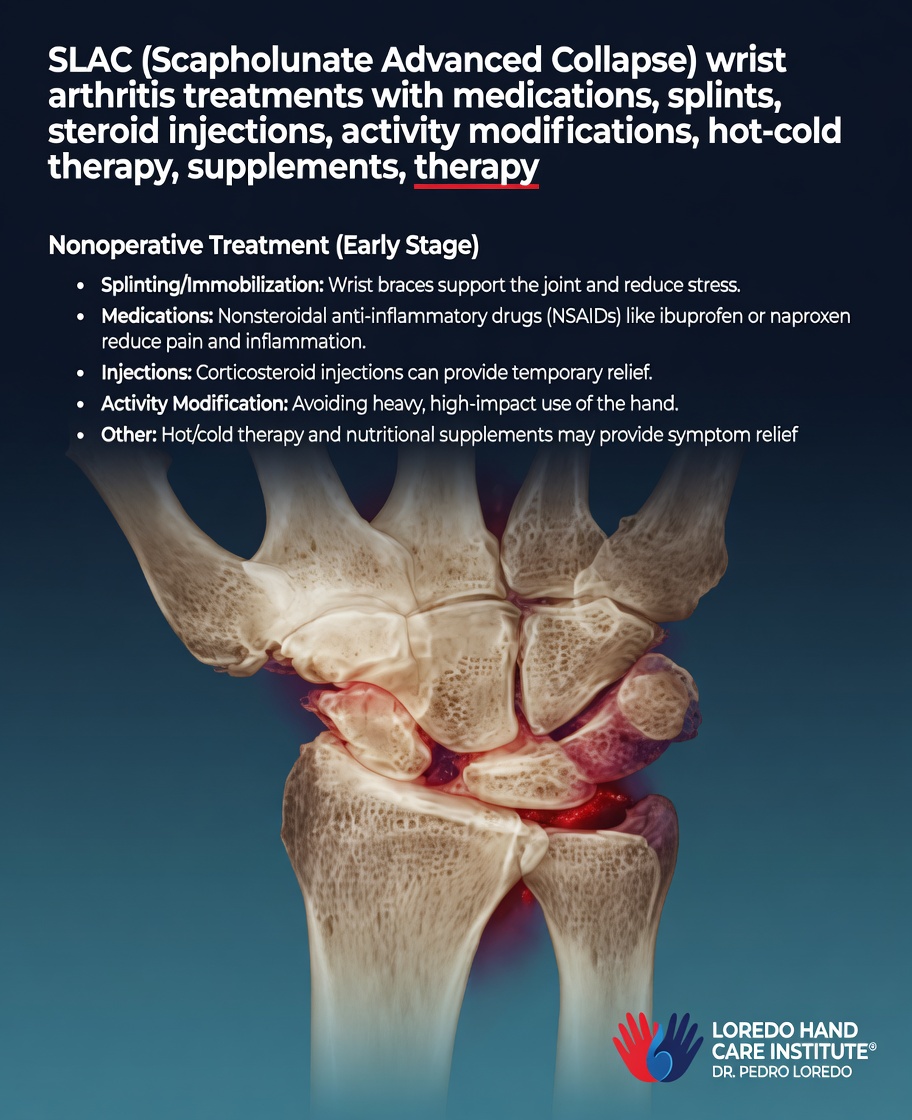
SLAC Wrist (Scapholunate Advanced Collapse)
SLAC wrist is a specific pattern of post-traumatic wrist arthritis that develops after an unrecognized or untreated scapholunate ligament injury. The torn ligament destabilizes the carpus, causing the scaphoid to rotate abnormally and load the joint surfaces unevenly. Over years, predictable cartilage wear progresses through three sequential stages.

SLAC Wrist Conservative Treatment
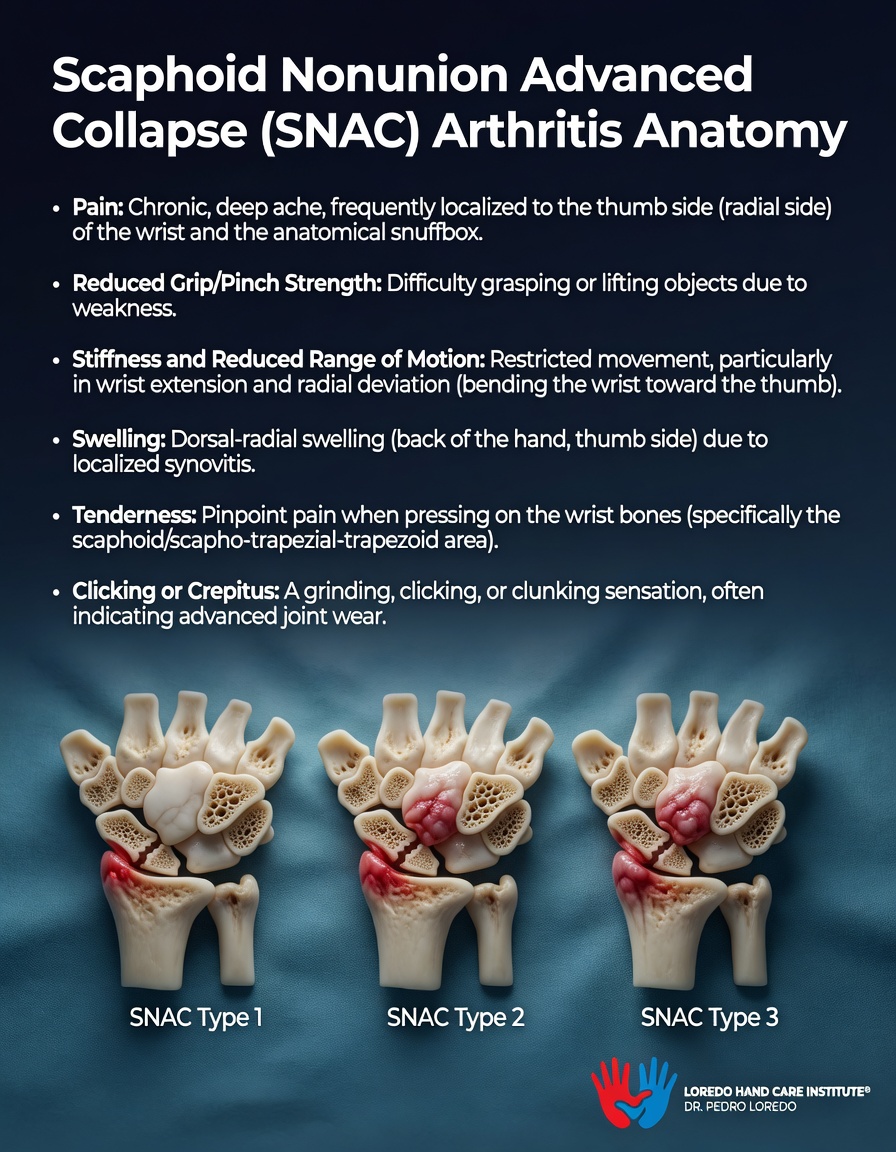
SNAC Wrist (Scaphoid Nonunion Advanced Collapse)
SNAC wrist is the post-traumatic arthritis pattern that develops after an unhealed (nonunion) scaphoid fracture. The persistent scaphoid fracture creates abnormal motion and uneven joint loading, producing predictable cartilage wear in three sequential types similar to SLAC but with distinct radiographic patterns.
SNAC Wrist Conservative Treatment

How the Diagnosis Is Made
Diagnosis combines a focused history, joint-by-joint examination, X-ray, and selective laboratory testing.
- History: timing, pattern of joint involvement, prior injury, family history, autoimmune disease.
- Physical exam: joint tenderness, swelling, warmth, deformity, range of motion, crepitus, nodules, ligamentous stability.
- X-ray: standard imaging. Joint space narrowing and osteophytes in OA. Erosions in RA. Old fracture or joint incongruity in post-traumatic disease.
- Laboratory testing: rheumatoid factor, anti-CCP antibodies, ESR, CRP when RA is suspected. ANA panel for lupus. Uric acid for gout.
- MRI is occasionally used to assess synovitis, soft-tissue involvement, or early erosions in RA when X-rays appear normal.
- Joint aspiration when crystal arthritis (gout, pseudogout) or septic arthritis is in the differential.
Non-Surgical Treatment Options
- Activity modification and joint protection education from a hand therapist
- Splinting, particularly for thumb CMC and wrist arthritis. Custom splints during aggravating tasks and at night.
- Hand therapy for range of motion, gentle strengthening, and ergonomic adaptation
- Topical and oral nonsteroidal anti-inflammatory medication
- Acetaminophen for patients who cannot tolerate NSAIDs
- Corticosteroid injection, most useful for thumb CMC, wrist, and selective PIP/DIP joints. Generally limited to 2 to 3 injections per joint per year.
- Disease-modifying antirheumatic drugs (DMARDs) and biologics for rheumatoid arthritis, prescribed and managed by a rheumatologist. These medications change the trajectory of RA and prevent the joint destruction that drives long-term hand deformity.

Surgical Options
Surgical treatment is matched to the affected joint, the stage of disease, and the patient's functional priorities. Dr. Loredo discusses each option in detail at consultation, including motion-preserving versus motion-eliminating choices.
Synovectomy
Surgical removal of inflamed synovial lining. Most useful in selected RA patients with persistent localized synovitis despite optimal medical therapy.
Finger Joint Surgery
Surgical treatment for arthritic finger joints (DIP and PIP) is matched to the specific joint and patient priorities. Fusion provides reliable pain relief by eliminating motion at the joint. Joint implants preserve motion at PIP joints.
Distal Interphalangeal (DIP) Joint Fusion
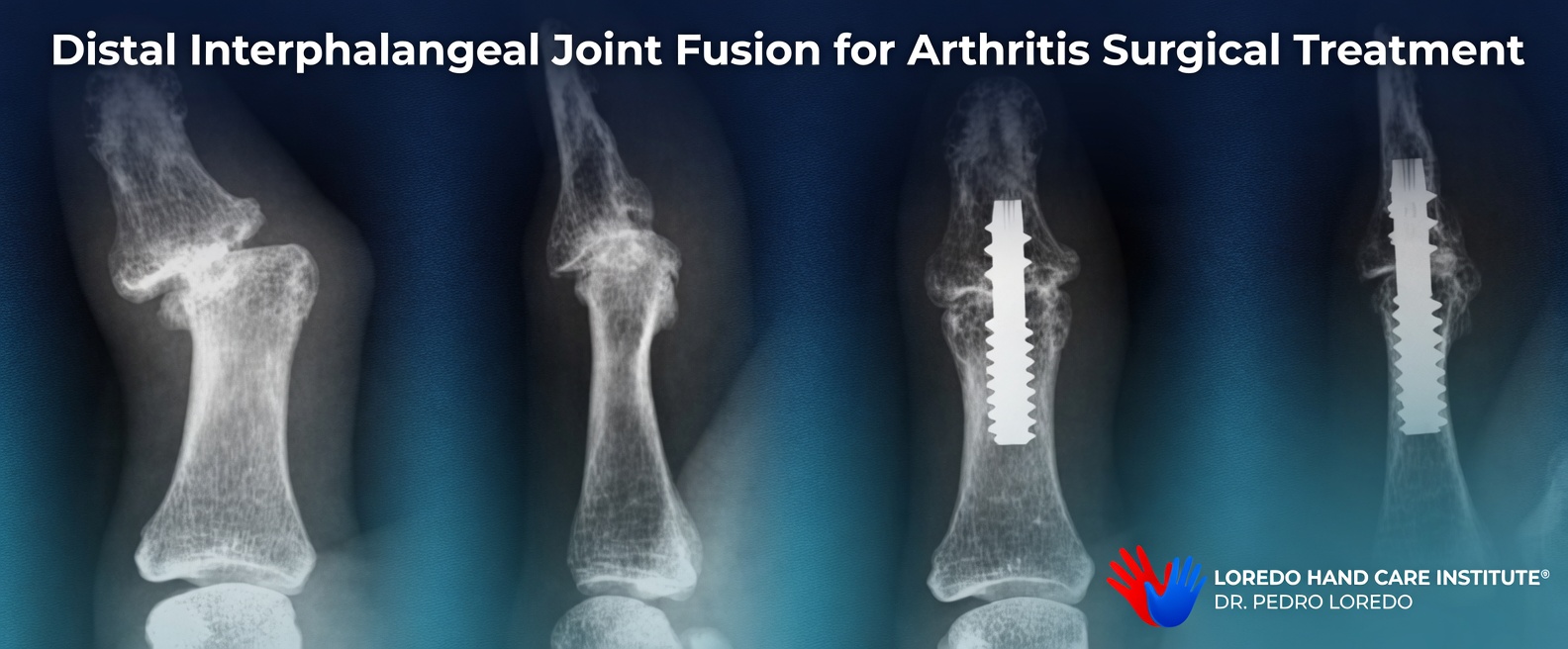
DIP fusion is the workhorse procedure for end-stage DIP joint arthritis. The DIP joint provides only fine-tuning motion, so fusion eliminates pain without meaningful functional loss. A small intramedullary screw or pin holds the joint surfaces together while bone heals across the joint.
Proximal Interphalangeal (PIP) Joint Fusion
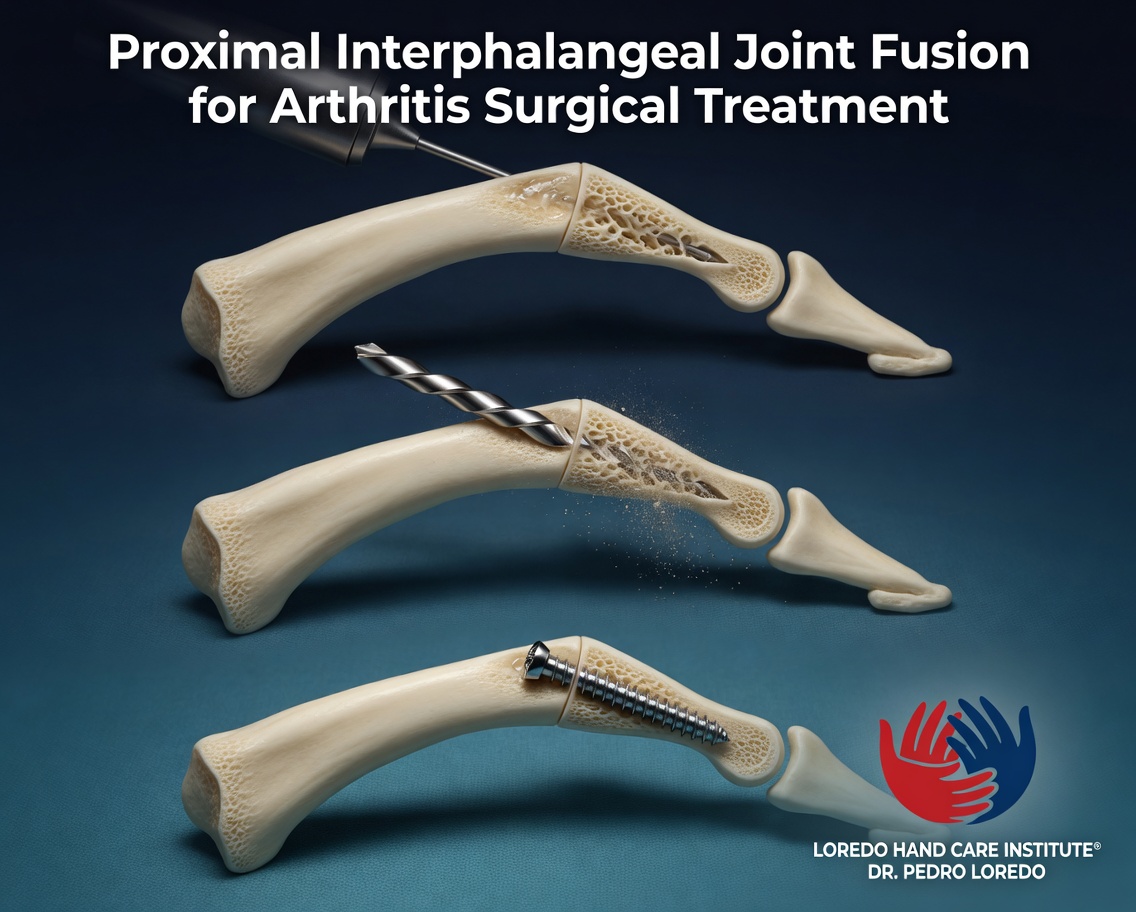
PIP fusion is selected for end-stage PIP arthritis when reliable pain relief and stability matter more than retained motion. Most often used at the index finger PIP joint where lateral pinch stability is critical, and at any PIP joint with severe deformity.
PIP Joint Implants (Arthroplasty)

PIP joint implant arthroplasty preserves motion at the PIP joint while eliminating the arthritic joint surfaces. Silicone and pyrocarbon are the two primary implant materials. Best suited for the middle, ring, and small finger PIP joints (motion preservation is more functionally important than at the index finger). Particularly useful in rheumatoid patients.
Wrist Arthritis Surgery

Early-Stage and Joint-Preserving Wrist Procedures
Radial Styloidectomy.
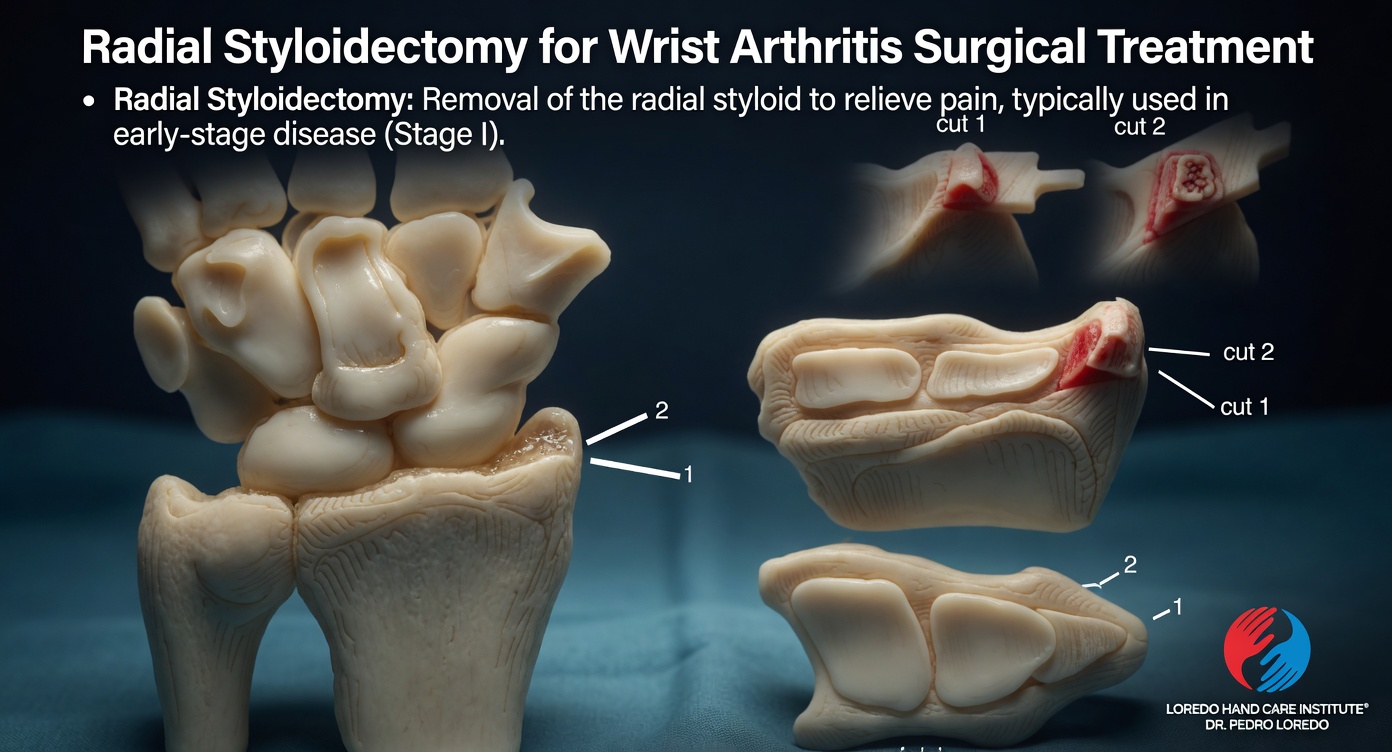
Removal of the radial styloid bone process to relieve impingement pain in early-stage (Stage I) SLAC or SNAC wrist disease. Often combined with other procedures.
Wrist Denervation.
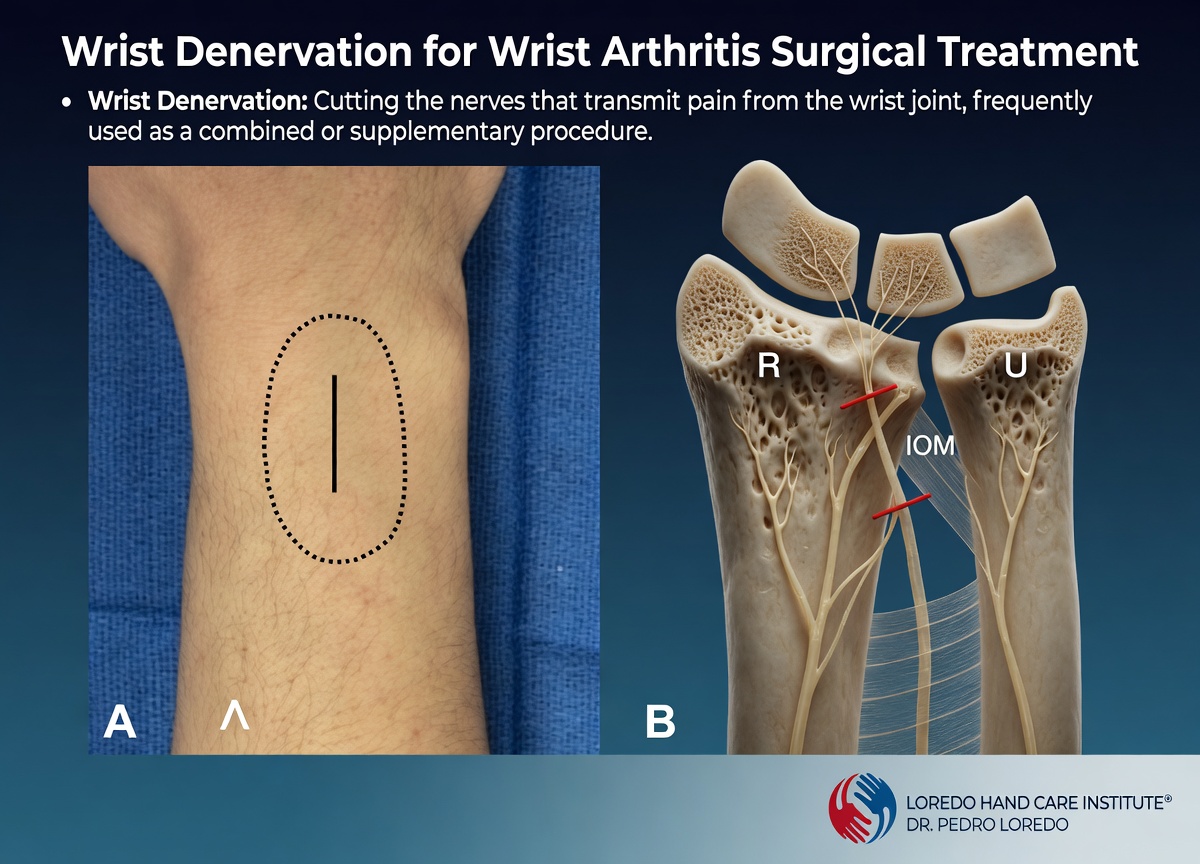
Selective division of the small sensory nerves that carry pain signals from the wrist joint. Preserves wrist motion completely. Used as a stand-alone procedure in select patients or combined with other procedures.
Distal Scaphoid Excision (SNAC-Specific).

Specific to SNAC wrist. Removes the distal portion of the unhealed scaphoid fragment that drives the abnormal joint motion and resultant arthritis. Preserves the proximal scaphoid and the rest of the wrist mechanics.
Motion-Preserving Wrist Reconstructions
Proximal Row Carpectomy (PRC).
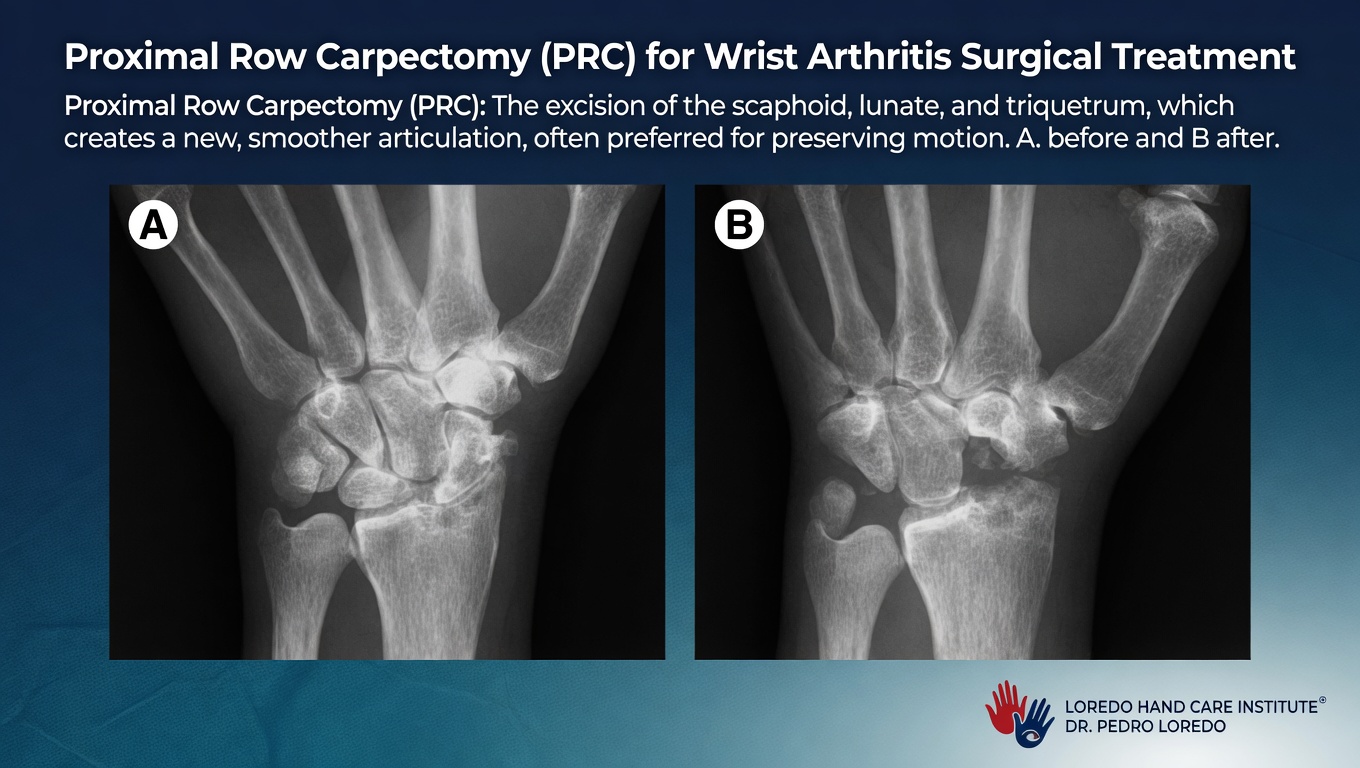
Excision of the scaphoid, lunate, and triquetrum (the entire proximal carpal row), allowing the capitate to articulate directly with the distal radius. Preserves substantial wrist motion. Best suited for older or lower-demand patients with intact radio-capitate cartilage. Recovery is faster than four-corner fusion.
Scaphoid Excision and Four-Corner Fusion (4CF).
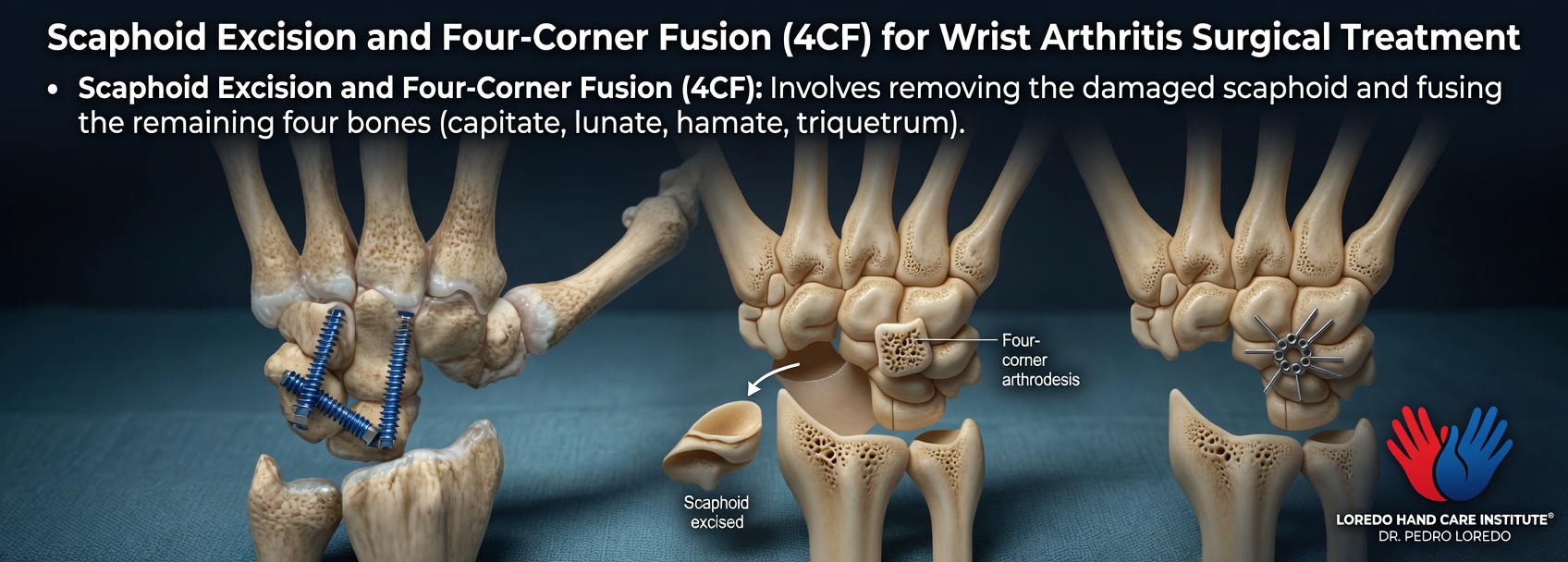
Removes the diseased scaphoid and fuses the remaining four bones of the proximal carpal row (capitate, lunate, hamate, triquetrum). Preserves the radiolunate articulation and approximately 50 to 60 percent of normal wrist motion. Provides reliable pain relief while maintaining functional motion. Often the preferred motion-preserving option for younger or higher-demand patients.
Salvage Procedures for End-Stage Wrist Arthritis
Total Wrist Arthrodesis (Total Wrist Fusion).
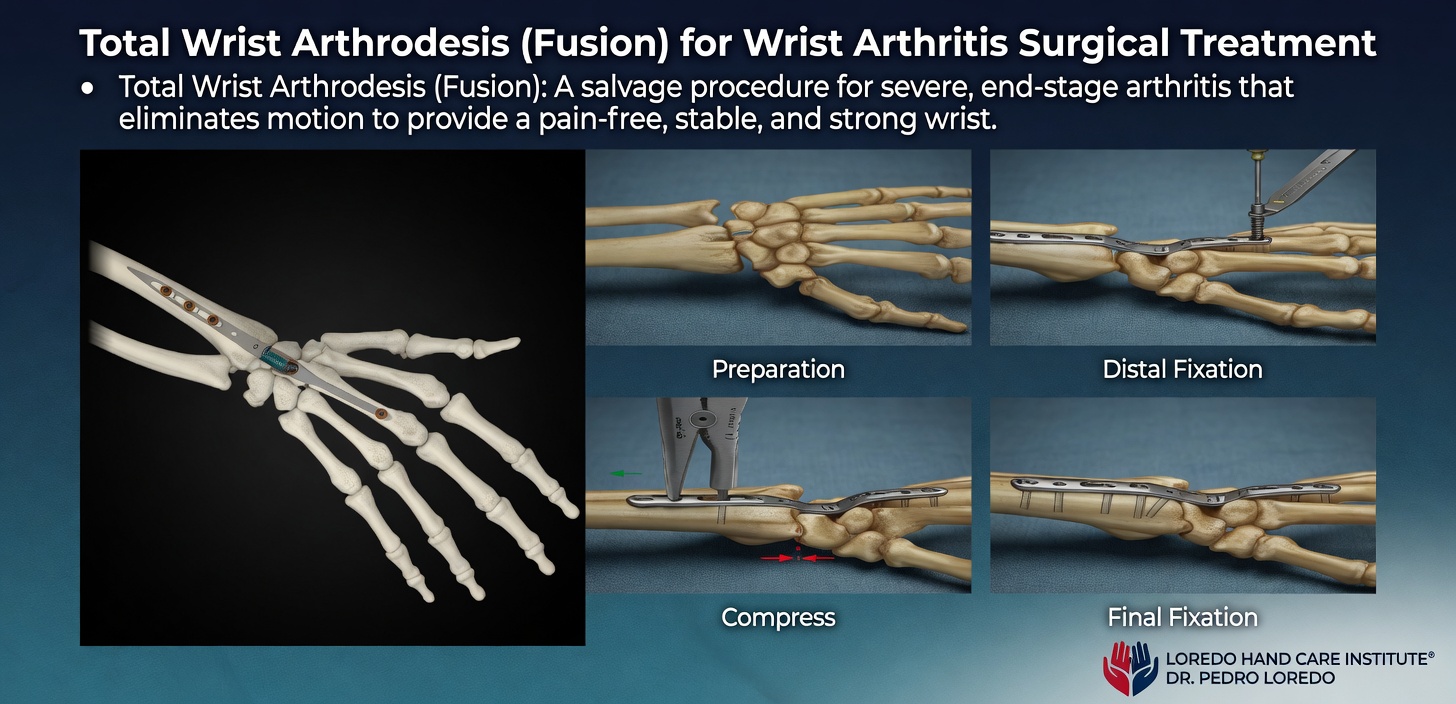
Salvage procedure for severe, end-stage wrist arthritis that eliminates motion to provide a pain-free, stable, and strong wrist. Best for high-demand laborers and patients who prioritize strength over motion. The wrist fuses in a slight extension position that maximizes hand function.
Total Wrist Arthroplasty (TWA).
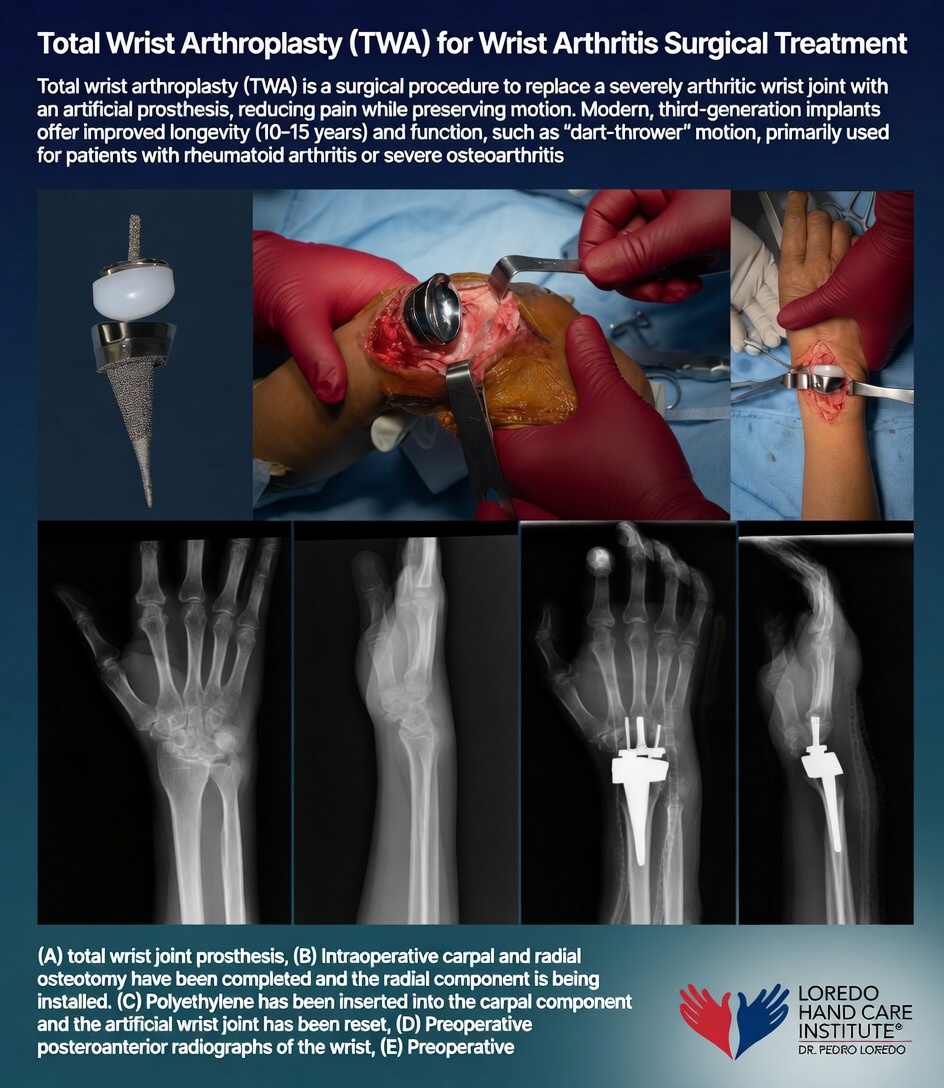
Replacement of the severely arthritic wrist joint with a modern third-generation prosthesis. Reduces pain while preserving motion (including the dart-thrower motion important for daily tasks). Modern implants offer 10 to 15 year longevity. Primarily used for rheumatoid arthritis patients or severe osteoarthritis patients who prioritize motion over the maximum durability of fusion.
Recovery Timeline
- Corticosteroid injection: same-day return to most activity. Pain relief begins within 24 to 72 hours.
- Synovectomy: 4 to 6 weeks of structured therapy. Custom splint as needed.
- MCP or PIP arthroplasty: 6 to 12 weeks of structured hand therapy with a custom splint and dynamic motion protocol.
- DIP or selective PIP fusion: 6 to 8 weeks in a finger splint until bony union is confirmed.
- Thumb CMC arthroplasty (LRTI): 4 weeks in a thumb spica splint, then 4 to 8 weeks of progressive therapy.
- Wrist procedures: 8 to 12 weeks in a cast or splint, then progressive therapy.
Returning to Work and Daily Activity
- Office or desk work in a removable splint: within days to a week after most procedures
- Light manual labor: 4 to 8 weeks depending on the operation
- Heavy manual labor: 12 to 16 weeks
- Driving: when grip strength and splint allow safe vehicle control, usually 2 to 6 weeks
Frequently Asked Questions
What is the difference between osteoarthritis and rheumatoid arthritis?
Osteoarthritis (OA) is mechanical wear-and-tear of joint cartilage. It usually starts after age 50, tends to be asymmetric, affects the fingertip and thumb-base joints most, and produces less than 30 minutes of morning stiffness. Rheumatoid arthritis (RA) is an autoimmune disease in which the immune system attacks the synovial lining of joints, eroding cartilage and bone. RA tends to be symmetric, affects the knuckle and wrist joints first, produces more than an hour of morning stiffness, and is diagnosed with blood tests showing rheumatoid factor and anti-CCP antibodies. The two conditions look similar on the outside but require very different treatment.
Are nodules at my fingertip joints serious?
Bony enlargements at the fingertip joints (DIP joints) are called Heberden's nodes and at the middle finger joints (PIP joints) are called Bouchard's nodes. They are a hallmark of osteoarthritis of the hand, appear over years, and are not dangerous. They can be unsightly and occasionally tender during a flare. Treatment focuses on managing pain, preserving function, and avoiding heavy gripping that aggravates the joints. Surgery is reserved for severely painful or unstable end-stage joints.
Does cracking my knuckles cause arthritis?
No. Multiple studies have looked specifically at this question and found no association between knuckle cracking and the development of arthritis. The popping sound is gas bubbles forming and collapsing within the joint fluid. It can become a habit, but it does not damage cartilage or accelerate joint wear.
When is joint replacement the right choice for hand arthritis?
Joint replacement (arthroplasty) is the right choice when joint pain is constant, conservative measures have failed, and motion preservation matters more than maximum stability. The MCP and PIP joints are the most common joints replaced in the hand, particularly in patients with rheumatoid arthritis. Thumb CMC arthritis is most often treated with trapezium excision and ligament reconstruction. Fusion (arthrodesis) is preferred at the DIP joint and for high-demand patients where pain relief and stability matter more than retaining motion.
Can hand arthritis be prevented?
Genetic risk for osteoarthritis cannot be changed. Post-traumatic arthritis can sometimes be prevented by prompt and accurate treatment of fractures and ligament injuries. Inflammatory arthritis is best prevented from progressing rather than from starting: early diagnosis and disease-modifying medication (managed by a rheumatologist) prevent the joint destruction that drives long-term hand deformity. For all forms, joint protection, regular activity, and avoiding tobacco are the most useful general measures.
When to Call the Doctor
Call our office for evaluation if you experience:
- Joint pain that has lasted more than several weeks
- Joint swelling that does not resolve within a week
- Morning stiffness lasting more than 30 minutes
- Symmetric joint involvement (suspect inflammatory arthritis)
- Loss of grip or pinch strength that limits work or daily life
- Visible joint deformity
- A sudden flare with redness, warmth, and severe pain (suspect crystal or septic arthritis)
After surgery, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the incision
- Thick, yellow, or foul-smelling drainage
- Severe pain not controlled by prescribed medication
- Sudden new finger numbness or inability to bend a finger
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Thumb Basilar Joint Arthritis: the most specific and common form of hand osteoarthritis. Treated as a dedicated condition because the thumb base has unique reconstructive options.
- Trigger Finger: often coexists with hand arthritis, particularly in patients with rheumatoid arthritis and diabetes.
- Carpal Tunnel Syndrome: frequently coexists with rheumatoid arthritis due to synovial swelling within the carpal tunnel.
- Hand and Finger Fractures: post-traumatic arthritis is a long-term consequence of fractures, particularly intra-articular distal radius and scaphoid nonunion.
- De Quervain's Tendonitis: can be confused with thumb CMC arthritis. Differentiated by exam and selective injection.
From the Blog
- Thumb Arthritis: When Injections Stop Working: the cortisone lifecycle for hand arthritis.
- The Basal Joint of the Thumb: why CMC arthritis is so common at the most-used joint.
- When a Cortisone Injection Is the Right Choice: response patterns by condition.
Watch: Hand arthritis education
Short videos from Dr. Loredo's Instagram and Facebook channels.