
Hand and finger fractures range from minor and forgiving to surgical emergencies that determine long-term hand function. The most common are distal radius fractures (a wrist break, often from falling on an outstretched hand), scaphoid fractures (a small carpal bone with a fragile blood supply that fails to heal in 10 to 25 percent of missed cases), boxer's fractures of the 5th metacarpal (typically from punching a hard object), and phalanx fractures of the finger bones. Treatment ranges from splinting and casting to closed reduction with percutaneous pinning and open reduction with internal fixation. Early evaluation matters: missed fractures, particularly scaphoid, can lead to chronic wrist arthritis years later.
The Anatomy of Hand and Wrist Bones
The hand and wrist contain 27 bones: 8 small carpal bones at the wrist, 5 metacarpals in the palm, and 14 phalanges in the fingers and thumb. The forearm contributes the radius and ulna, both of which articulate with the carpal bones at the wrist. Each fracture is named for the specific bone and the specific location within the bone, because each pattern has its own healing behavior and treatment options.
Clinical coding: ICD-10 S52.5 (distal radius), S62.0 (scaphoid), S62.3 (other and unspecified metacarpal), S62.6 (phalanx). SNOMED CT 125605004 (fracture of bone).
Common Fracture Patterns

Distal Radius Fracture
The most common fracture in adults. Typically caused by a fall on an outstretched hand. Can range from a stable nondisplaced crack to a comminuted intra-articular pattern that disrupts the wrist joint surface. Treatment depends on displacement, joint involvement, and patient demands. Closed reduction and casting works for many. Volar locking plate fixation is the most common surgical option for unstable patterns and provides reliable early motion.
Scaphoid Fracture
The scaphoid is a small carpal bone at the base of the thumb. It receives most of its blood supply from a single artery that enters at the distal end and runs back through the bone in a retrograde direction. A fracture across the middle (waist) of the scaphoid can cut off blood supply to the proximal half. Without prompt and correct treatment, the proximal scaphoid can fail to heal (nonunion) or die (avascular necrosis), leading to a predictable pattern of wrist arthritis years later. Suspicion alone (pain in the anatomic snuffbox after a fall on an outstretched hand) warrants splinting and re-evaluation even when the initial X-ray is negative.
Boxer's Fracture (5th Metacarpal Neck)
Fracture of the neck of the 5th metacarpal, the bone behind the small finger knuckle. Typically results from punching a hard object. Most boxer's fractures heal well with closed treatment in a splint or short cast for 3 to 4 weeks. Surgery is considered when angulation is greater than 40 degrees, when there is rotational malalignment causing finger overlap on a fist, or in high-demand hand users who cannot tolerate residual deformity.
Phalanx Fractures
Fractures of the proximal, middle, or distal phalanx of any finger. Most are stable and heal with buddy-taping or a finger splint for 3 to 4 weeks. Spiral, oblique, or intra-articular patterns may require percutaneous pinning or open reduction. Rotational deformity is the unforgiving variable: a finger that rotates even a few degrees can cross over its neighbor when the fist is closed and is a clear surgical indication.
Causes and Risk Factors
- Falls on an outstretched hand are the leading cause of distal radius and scaphoid fractures
- Direct blow to the hand, including punching injuries (boxer's fractures)
- Sports injuries: skiing, snowboarding, cycling, contact sports, basketball, and football
- Motor vehicle collisions
- Crush injuries at work or home
- Osteoporosis, which lowers the energy required to produce a fracture in older adults
- Smoking, which delays bone healing
Symptoms and Warning Signs
- Pain and tenderness localized to a specific bone or region
- Bruising and swelling, sometimes delayed by hours
- Visible deformity or angulation, including a depressed knuckle in boxer's fractures
- Inability to grip, write, or perform fine pinch tasks
- Pain in the anatomic snuffbox at the base of the thumb (suspect scaphoid)
- Finger overlap when making a fist, suggesting rotational deformity
- Numbness or tingling, which may indicate associated nerve compression
How the Diagnosis Is Made
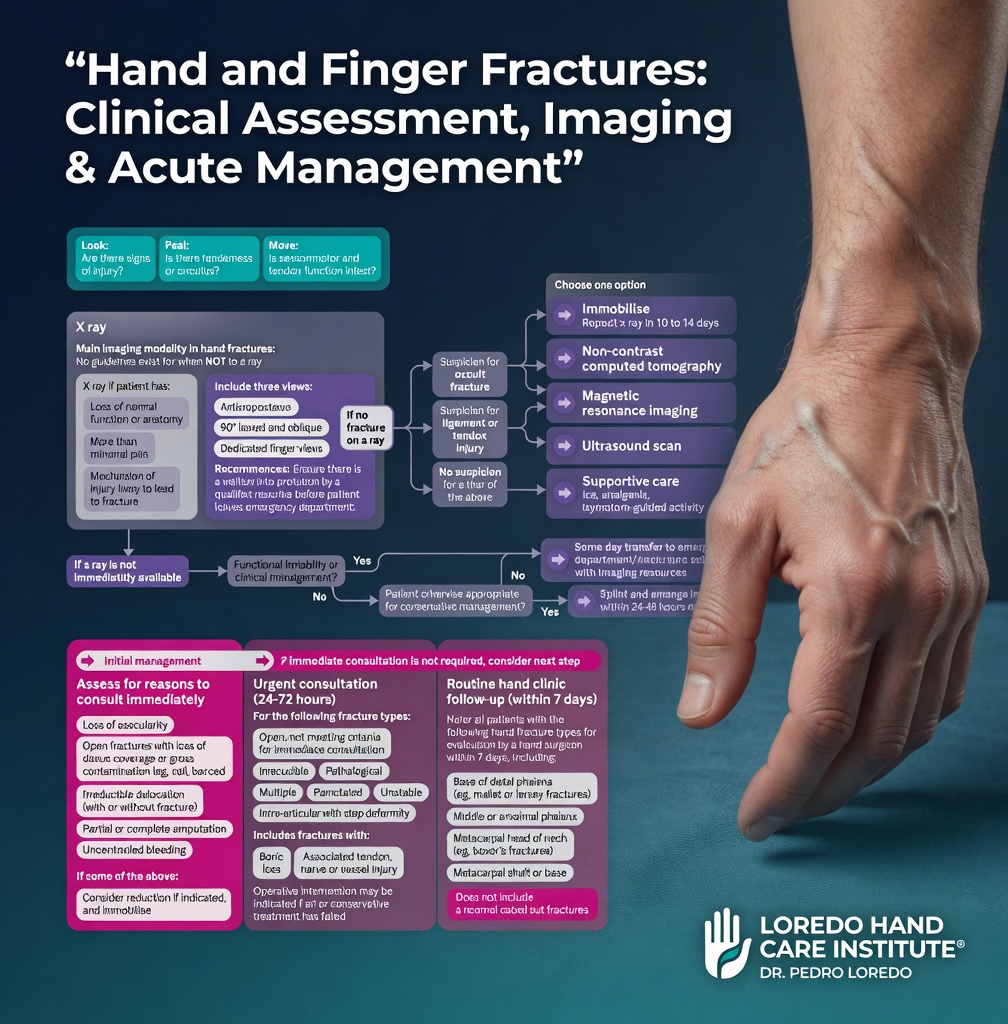
The evaluation begins with a focused history and a careful examination that localizes tenderness to a specific bone, assesses for rotational alignment of the fingers, and rules out tendon or nerve injury.
- X-ray: standard first imaging. Three views (PA, lateral, oblique) are obtained for most hand and wrist injuries.
- Scaphoid views: dedicated views with the wrist in ulnar deviation when scaphoid fracture is suspected.
- CT scan: helpful for occult scaphoid fractures, articular distal radius fractures, and complex carpal injuries.
- MRI: the most sensitive test for occult scaphoid fracture and for evaluating ligament injuries that often accompany fractures.
- Repeat imaging in 10 to 14 days when the initial X-ray is negative but clinical suspicion is high. The fracture line often becomes visible as the bone resorbs at the fracture edges.
Treatment Options
Non-Surgical Treatment

- Splinting or casting for stable, nondisplaced fractures, typically for 3 to 6 weeks depending on the bone
- Closed reduction under local or hematoma block for displaced but reducible fractures, followed by casting
- Buddy-taping for stable phalanx fractures of an adjacent uninjured finger
- Hand therapy initiated as soon as the fracture is stable enough to allow protected motion
Surgical Treatment
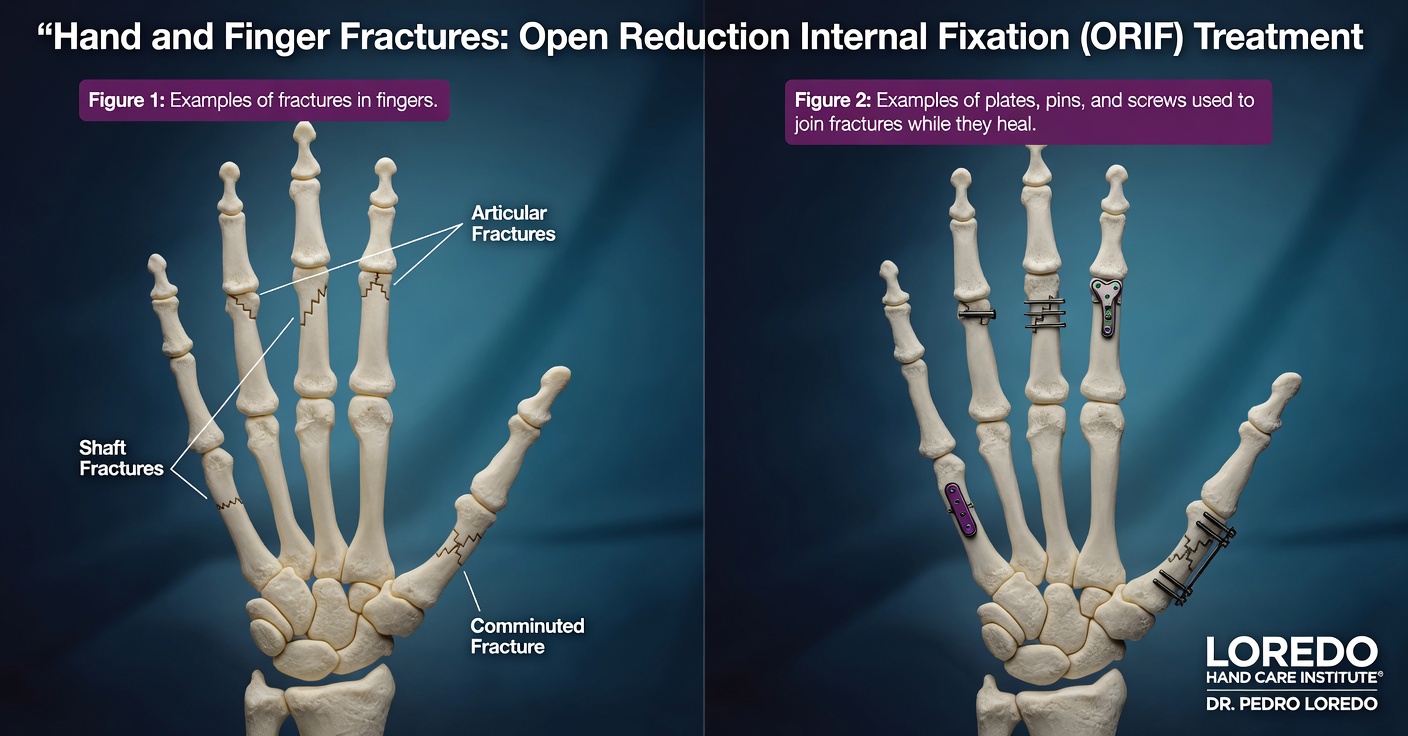

- Percutaneous pinning with K-wires for fractures that can be reduced closed but require fixation
- Open reduction and internal fixation (ORIF) with plates and screws, the workhorse for most displaced and unstable fractures
- Scaphoid screw fixation for displaced scaphoid fractures, often through a small percutaneous approach
- External fixation for severely comminuted distal radius fractures or open injuries
- Bone grafting in scaphoid nonunion or complex multi-fragment fractures
Recovery Timeline
- Phalanx and metacarpal fractures: 4 to 6 weeks for bone healing, with hand therapy starting at week 2 to 3 to maintain motion
- Distal radius fractures: 6 to 8 weeks for bone healing. Volar plate fixation often allows protected motion within 1 to 2 weeks of surgery.
- Scaphoid fractures: 8 to 12 weeks for bone healing. Some scaphoid fractures take longer and a small percentage require additional surgery for nonunion.
- Functional recovery beyond bone healing typically takes an additional 6 to 12 weeks for grip strength and full range of motion.
Returning to Work and Daily Activity
- Office or desk work in a removable splint: within days for most stable patterns
- Light manual labor: 4 to 8 weeks, depending on the bone and fixation method
- Heavy manual labor: 8 to 16 weeks
- Driving: when the cast or splint is removed and grip strength is adequate, usually 2 to 6 weeks
- Contact sports and weightlifting: 3 to 6 months depending on the bone and fixation
Frequently Asked Questions
How do I know if my hand is broken or just badly bruised?
You usually cannot reliably tell from the outside. Bruising, swelling, and pain are common to both. Inability to grip, visible deformity, or pain that does not improve over 48 hours after a clear injury are reasons to get an X-ray. Some fractures, including scaphoid and small finger phalanx fractures, can produce surprisingly little swelling early on but have serious long-term consequences if missed. When in doubt, get the X-ray.
Why is a scaphoid fracture so important to catch early?
The scaphoid bone receives most of its blood supply from a single artery that enters at the distal end and runs back through the bone in a retrograde direction. A fracture across the middle (waist) of the scaphoid can cut off blood supply to the proximal half. Without prompt and correct treatment, the proximal scaphoid can fail to heal (nonunion) or die (avascular necrosis), leading to wrist arthritis years later. Any pain in the anatomic snuffbox after a fall on an outstretched hand should be evaluated even when the X-ray initially appears normal, because scaphoid fractures are missed on first X-rays in 10 to 25 percent of cases.
What is a boxer's fracture and does it always need surgery?
A boxer's fracture is a fracture of the neck of the 5th metacarpal, the bone behind the small finger knuckle. It typically results from punching a hard object. Most boxer's fractures heal well with closed treatment in a splint or short cast for 3 to 4 weeks. Surgery is considered when angulation is greater than 40 degrees, when the fracture is rotated (causing finger overlap when making a fist), or when the patient is a high-demand hand user. The depressed knuckle may remain even after the bone heals, which is cosmetic but not functional.
How long does a hand fracture take to heal?
Bone healing in the hand typically takes 4 to 6 weeks for phalanx and metacarpal fractures, 6 to 8 weeks for distal radius fractures, and 8 to 12 weeks for scaphoid fractures. Functional recovery, including grip strength and full range of motion, takes longer than bone healing alone. Most patients regain near-full function within 3 to 4 months. Stiffness is the most common long-term issue and is minimized with early protected motion and structured hand therapy.
Will my hand work normally again after a fracture?
Most simple closed hand and finger fractures heal with excellent functional outcomes when treated early and correctly. Complex fractures involving the joint surface, fractures with significant displacement, fractures with associated tendon or nerve injury, and fractures that go untreated for weeks have a higher risk of stiffness, persistent weakness, or post-traumatic arthritis. Hand therapy is a key part of recovery in nearly every fracture and is what separates a stiff hand from a fully functional one.
When to Call the Doctor
Call our office promptly if you experience:
- Hand, wrist, or finger pain after a fall, blow, or twisting injury
- Inability to grip or use the hand normally after an injury
- Visible deformity, depressed knuckle, or finger that crosses over its neighbor on a fist
- Pain in the anatomic snuffbox at the base of the thumb after a fall on an outstretched hand (suspect scaphoid)
- Pain that has not improved after 48 to 72 hours from a clear injury
- New numbness, tingling, or weakness in any finger after an injury
After fracture treatment, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness, warmth, or drainage around any incision
- Severe pain that is not controlled by prescribed medication
- New numbness, tingling, or color change in the fingers
- A cast that is too tight or that cracks, breaks, or gets wet
Open fractures (bone exposed through the skin), deformities with skin compromise, or signs of compartment syndrome (severe pain out of proportion, tense swelling, finger numbness) are emergencies. Call 911 or go to the nearest emergency department immediately.
Related Conditions
- Hand and Wrist Arthritis: post-traumatic arthritis is a long-term consequence of poorly healed or untreated fractures, particularly scaphoid nonunion and intra-articular distal radius fractures.
- Carpal Tunnel Syndrome: acute carpal tunnel syndrome can develop after a distal radius fracture due to pressure in the carpal tunnel from displacement and swelling.
- Dupuytren's Contracture: prior trauma occasionally unmasks early Dupuytren's disease in genetically predisposed patients.
- Trigger Finger: occasionally develops months after a hand injury due to local inflammation around a flexor tendon.
- Thumb Basilar Joint Arthritis: can develop after thumb metacarpal fractures that involved the joint surface.
From the Blog
- Distal Radius Fractures: Should You Get Surgery?: cast versus volar locking plate.
- Scaphoid Fractures: Why They Are Dangerous: retrograde blood supply and SNAC wrist progression.
- Why Same-Week Hand Surgery Matters: time-sensitive injuries that get worse with delay.
Watch: Hand fracture education
Short videos from Dr. Loredo's YouTube and Facebook channels.