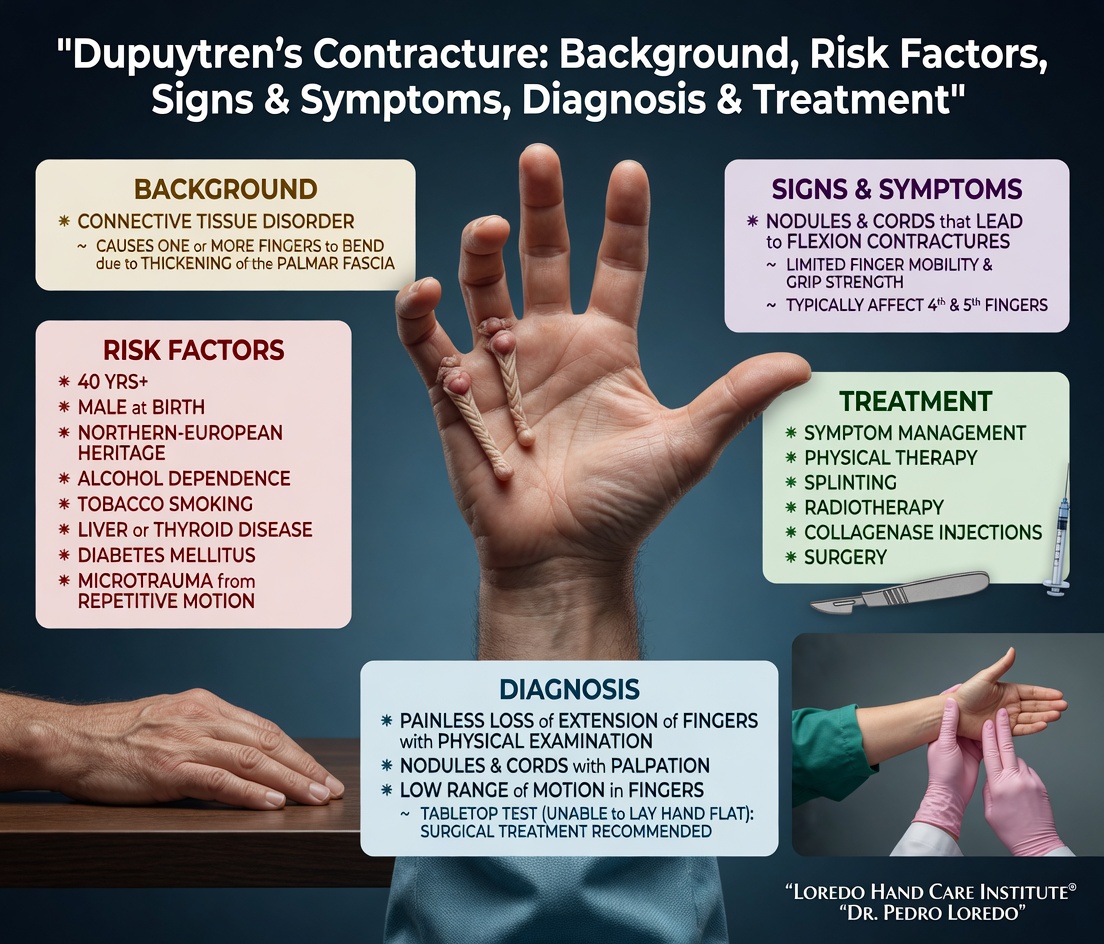
Dupuytren's contracture is a benign but progressive thickening and shortening of the palmar fascia, the connective tissue layer just beneath the skin of the palm. Cords of fascia pull one or more fingers, most often the ring and small fingers, into a fixed flexed position that cannot be passively straightened. Treatment is staged: observation in early disease, needle aponeurotomy or collagenase (Xiaflex) injection in moderate disease, and open fasciectomy in severe or recurrent disease. Dupuytren's tends to recur over years and is managed as a chronic condition rather than a curable one.
The Anatomy of the Palmar Fascia
The palmar fascia is a thin tough sheet of connective tissue that lies between the skin of the palm and the flexor tendons. It extends from the wrist into each finger and helps anchor the skin during gripping. In Dupuytren's disease, fibroblasts within this fascia begin to proliferate and lay down disorganized collagen, forming first a small nodule and then a linear cord. Over months to years, the cord contracts and pulls the affected finger into the palm.
The disease most commonly affects the ring and small fingers because the fascial bands serving those digits are most prominent. The middle finger is involved less often, and the index and thumb only rarely. Dupuytren's affects men more than women, and most patients are over 50 at presentation. There is a strong genetic component: about 70 percent of patients have a family history. Patients of Northern European descent are most commonly affected, hence the historical name "Viking disease."
Clinical coding: ICD-10 M72.0 (palmar fascial fibromatosis, Dupuytren's). SNOMED CT 80131001.
Causes and Risk Factors
- Genetic predisposition with family history in roughly 70 percent of cases
- Northern European ancestry (Viking disease)
- Male sex (more common, more severe, earlier onset than in women)
- Age over 50
- Diabetes, particularly long-standing
- Tobacco use
- Chronic alcohol use
- Possible association with manual labor, though the evidence is mixed
Trauma may unmask early disease but does not cause it. Dupuytren's is not contagious and is not a cancer.
Symptoms and Warning Signs
- Painless palm nodule, often near the base of the ring or small finger
- Skin pitting or dimpling overlying the nodule
- Thickening of a linear band (cord) extending from the palm into a finger
- Inability to lay the palm flat on a tabletop
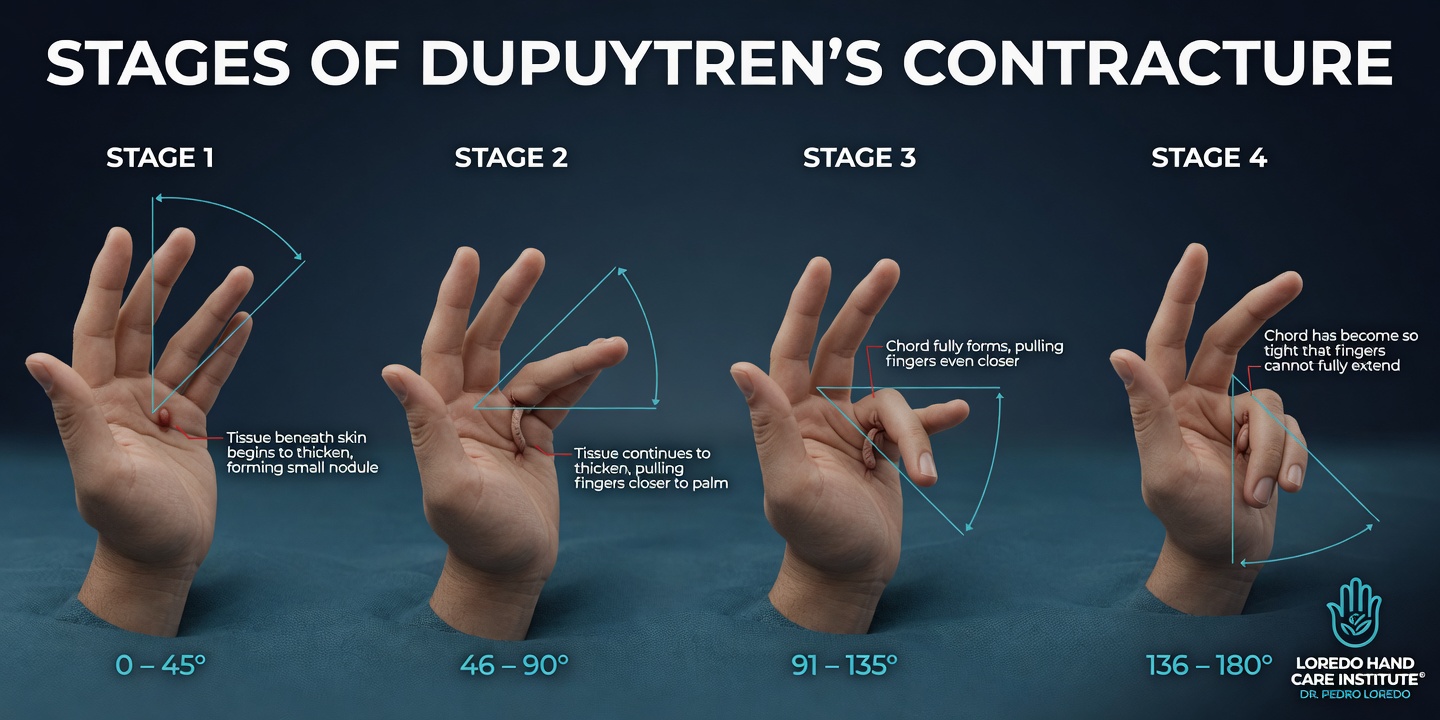
- Progressive flexion contracture of metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints
- Difficulty washing the face, putting the hand in a pocket, or shaking hands
- Bilateral involvement in many cases, often more advanced on the dominant hand
How the Diagnosis Is Made
Dupuytren's is a clinical diagnosis. Examination findings carry the diagnosis without the need for imaging in nearly all cases.
- Inspection and palpation: visible or palpable nodules and cords in the palm and digits, with characteristic skin pitting overlying nodules.
- Hueston tabletop test: the patient lays the hand flat on a tabletop. If the palm cannot rest flat against the surface because one or more fingers will not straighten, the test is positive. A positive tabletop test is the most common functional indication for procedure-based treatment.
- Goniometer measurement of MCP and PIP joint contracture in degrees, tracked at each visit to monitor progression.
The differential includes trigger finger (which has a tendon nodule, not fascial), ganglion cyst (fluid-filled rather than fibrous), and localized scar tissue from prior trauma.
Non-Surgical Management
- Observation in early disease without significant contracture. Many patients have stable mild disease for years.
- Hand therapy and stretching: limited evidence to slow progression, but useful in maintaining range of motion in mild disease.
- Splinting: does not prevent disease progression and is not a primary treatment.
- Steroid injection into early painful nodules can flatten the nodule and reduce tenderness but does not address established cords.
Procedure-Based Treatment
Needle Aponeurotomy (Percutaneous Needle Fasciotomy)
- Office procedure under local anesthesia
- A sterile needle is used to perforate and weaken the cord at multiple points along its length
- Gentle finger extension then ruptures the cord
- Skin remains intact, no incision, no sutures
- Best for cords with predominant MCP joint contracture
- Recurrence rate: 50 to 70 percent over 5 years
Collagenase Clostridium histolyticum (Xiaflex) Injection
- Outpatient injection of collagenase enzyme directly into the cord
- 24 to 48 hours later, the cord is manipulated to rupture and the finger is extended
- Best for cords with predominant MCP joint contracture
- Recurrence rate similar to needle aponeurotomy
- Mild bruising and swelling for 1 to 2 weeks afterward
Open Palmar Fasciectomy

- Operating room procedure under regional or general anesthesia
- Zigzag (Brunner) incision over the affected palm and finger
- Surgical removal of the diseased cord with careful preservation of the digital nerves and arteries that often run within or beneath it
- Skin closure or skin grafting if skin is too thin or too tight to close primarily
- Best for severe contracture, PIP joint involvement, recurrent disease, or younger patients with aggressive disease
- Recurrence rate: 20 to 40 percent over 5 to 10 years (lower than needle or Xiaflex)
Recovery Timeline
- Needle aponeurotomy: same-day return to most light activity. Mild bruising for 1 to 2 weeks. Hand therapy is optional. Driving same day or next day.
- Xiaflex: 1 to 2 weeks of mild swelling and bruising. Night splinting for about 4 weeks to maintain extension. Hand therapy as needed.
- Open fasciectomy: dressing for 1 week, followed by 6 to 12 weeks of structured hand therapy. Custom night extension splint, edema control, scar management. Driving in 1 to 2 weeks. Office work in 1 to 2 weeks. Manual labor in 6 to 12 weeks.
Returning to Work and Daily Activity
- Office or desk work: next day after needle or Xiaflex; 1 to 2 weeks after fasciectomy
- Light manual labor: 1 to 2 weeks after needle or Xiaflex; 4 to 6 weeks after fasciectomy
- Heavy manual labor: 2 to 4 weeks after needle or Xiaflex; 8 to 12 weeks after fasciectomy
- Driving: same day to next day for needle/Xiaflex; 1 to 2 weeks after fasciectomy
Frequently Asked Questions
Can Dupuytren's go away on its own?
No. Once nodules and cords are established, the fibrous tissue does not regress spontaneously. Some patients have stable mild disease for years that never progresses to a significant contracture. Others progress steadily and lose function within 1 to 2 years of onset. Observation is reasonable in early disease without functional impairment.
What is the Hueston tabletop test?
Place your hand flat on a table, palm down, with fingers fully extended. If the palm cannot rest flat against the table because one or more fingers will not straighten, the test is positive. A positive tabletop test is the most common functional indication for procedure-based treatment because at that point the contracture is interfering with daily tasks.
Will Dupuytren's come back after treatment?
Often yes. Dupuytren's is a chronic condition, not a curable one. Recurrence rates over 5 years are 50 to 70 percent after needle aponeurotomy or Xiaflex and 20 to 40 percent after open fasciectomy. We treat the condition rather than cure it. The goal is to restore function, accept that some recurrence is likely, and treat each new episode as it appears.
How do I choose between needle, Xiaflex, and surgery?
The right answer depends on which joint is involved, the severity of the contracture, your age, occupation, and your tolerance for downtime. Needle and Xiaflex are office-based with rapid recovery and are ideal for moderate MCP-predominant contracture. Open fasciectomy is the most durable and is the right choice for severe disease, PIP joint involvement, or recurrent disease. We work through the options together.
Will Dupuytren's affect my other hand or feet?
Often yes. About half of patients eventually develop disease on both hands. A related condition called Ledderhose disease affects the plantar fascia of the feet and occurs in 5 to 25 percent of Dupuytren's patients. Peyronie's disease, which affects the penis, also shares the same genetic background.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- Inability to lay the palm flat on a table
- Fingers progressively contracting toward the palm
- A new painful nodule in the palm or finger
- Loss of finger extension over months
- Recurrent disease after a previous treatment
After any procedure, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the procedure site
- Thick, yellow, or foul-smelling drainage
- Severe pain not controlled by prescribed medication
- Sudden new finger numbness or inability to bend the finger
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Trigger Finger: a different palmar problem (a tendon nodule, not fascial) that can coexist with Dupuytren's, especially in diabetic patients.
- Carpal Tunnel Syndrome: occasionally coexists with Dupuytren's. Both are more common in patients with diabetes.
- Hand and Wrist Arthritis: arthritic joint stiffness can be confused with Dupuytren's contracture in early disease. Imaging and a skilled exam separate them.
- Hand and Finger Fractures: prior trauma occasionally unmasks early Dupuytren's disease in genetically predisposed patients.
- Cubital Tunnel Syndrome: ulnar nerve compression that produces ring and small finger symptoms that some patients confuse with Dupuytren's contracture early on.
From the Blog
- Dupuytren Injection vs Needle vs Surgery: three modern treatment options compared.
- Hand Therapy After Surgery: what to expect from a Certified Hand Therapist.
Watch: Dupuytren's contracture education
Short videos from Dr. Loredo's Instagram and Facebook channels.