
Golfer's elbow, or medial epicondylitis, is a degenerative tendinopathy of the flexor-pronator tendon group at the inside of the elbow. The hallmark is pain at the bony bump on the inner elbow that worsens with gripping, throwing, or wrist flexion. Most cases respond to activity modification, counterforce bracing, eccentric forearm flexor strengthening, and time. Persistent cases that resist conservative care for 6 to 12 months may warrant corticosteroid injection, platelet-rich plasma, or surgical debridement of the flexor-pronator tendon origin.
The Anatomy of the Medial Elbow
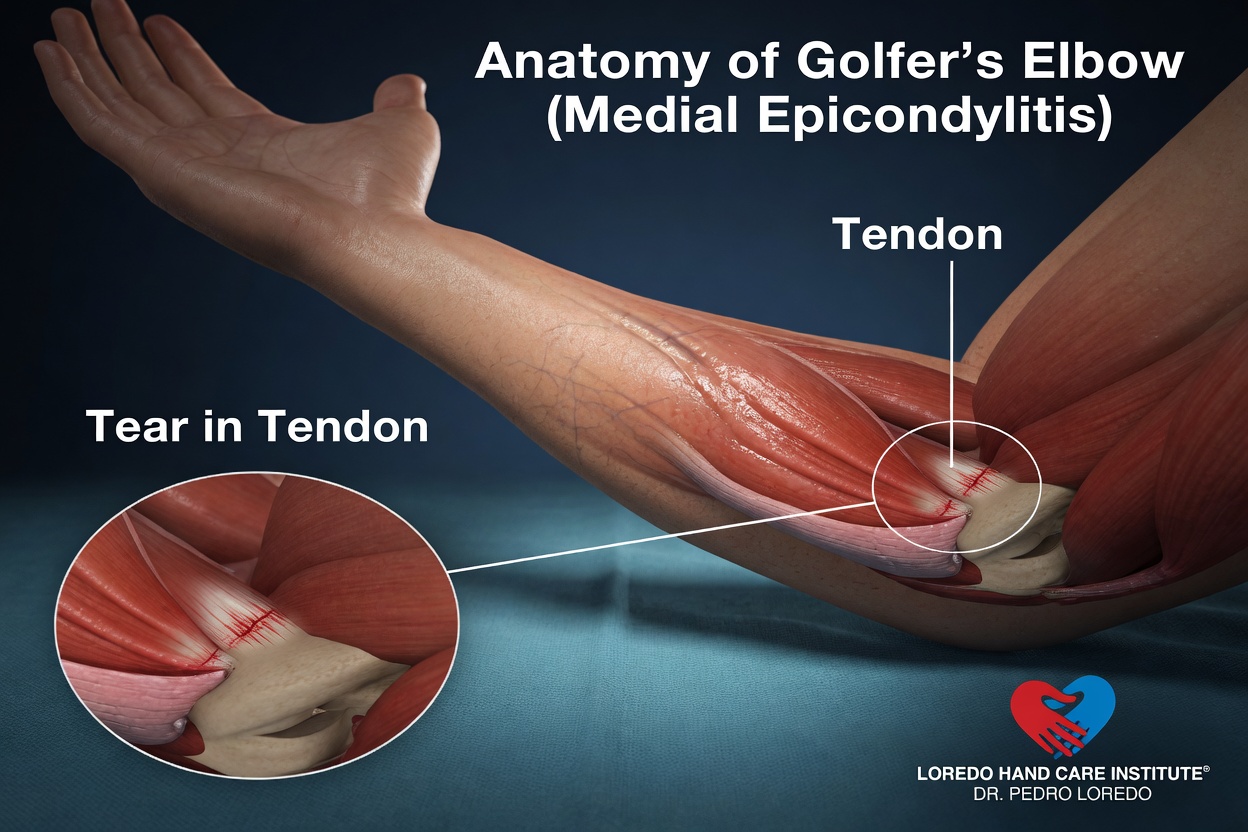
The medial epicondyle is the bony bump on the inside of the elbow at the end of the humerus. It is the shared origin point for the muscles of the flexor-pronator group: the pronator teres, the flexor carpi radialis, the palmaris longus, the flexor digitorum superficialis, and the flexor carpi ulnaris. These muscles flex the wrist and pronate the forearm. The pathology in golfer's elbow most commonly affects the pronator teres and flexor carpi radialis tendons at their attachment to bone.
The ulnar nerve runs through the cubital tunnel directly behind the medial epicondyle. Roughly 20 to 30 percent of patients with chronic golfer's elbow have coexisting ulnar nerve symptoms, which is why a careful examination always assesses both the medial tendon origin and the nerve. As with tennis elbow, the underlying pathology is angiofibroblastic degeneration rather than active inflammation, and treatment principles emphasize load management and eccentric strengthening over anti-inflammatories.
Clinical coding: ICD-10 M77.00 (medial epicondylitis). SNOMED CT 202855007.
Causes and Risk Factors
Golfer's elbow is an overuse condition. Common contributors:
- Repetitive wrist flexion and gripping at work or in sport
- Throwing sports including baseball pitching and javelin
- Golf, particularly with mechanical errors that load the trail arm
- Manual labor: hammering, screwing, repetitive lifting
- Weight training with heavy gripping and pulling movements
- Smoking and diabetes, which impair tendon healing
- Age 35 to 55
Despite the name, fewer than half of patients with medial epicondylitis play golf. The condition is just as common in pitchers, weightlifters, and manual workers.
Symptoms and Warning Signs
- Pain at the bony bump on the inside of the elbow
- Pain that radiates down the inside of the forearm toward the wrist
- Pain on gripping, lifting with the palm up, or twisting motions like opening a jar
- Weakness with squeezing, twisting, or pulling
- Tenderness on direct pressure over the medial epicondyle, slightly anterior and distal
- Stiffness in the morning that loosens with activity
- Coexisting tingling or numbness in the ring and small fingers (suggests ulnar nerve involvement)
How the Diagnosis Is Made
Golfer's elbow is a clinical diagnosis. Dr. Loredo performs three standard examination components:
- Resisted wrist flexion test: the standard provocative test. With the elbow extended and forearm supinated, the patient flexes the wrist against the examiner's resistance. Reproduction of pain at the medial epicondyle is positive.
- Resisted forearm pronation: with the elbow at 90 degrees, the patient pronates against resistance. Pain at the medial epicondyle implicates the pronator teres origin specifically.
- Tinel's sign at the cubital tunnel: tapping over the ulnar nerve behind the medial epicondyle. Tingling into the ring and small fingers indicates ulnar nerve irritation, which often coexists with medial epicondylitis.
Imaging is not always required. X-ray rules out joint pathology, calcification, or arthritis. Ultrasound or MRI confirms tendinopathy and grades severity when symptoms persist or surgery is contemplated. Nerve conduction studies are added when cubital tunnel syndrome is suspected.
Non-Surgical Treatment Options

Roughly 80 percent of cases resolve within 6 to 12 months with consistent conservative care.
- Activity modification: swing assessment for golfers, throwing mechanics review for pitchers, lifting technique adjustment for manual workers.
- Counterforce brace worn 1 to 2 inches distal to the medial epicondyle during aggravating activities.
- Targeted physical therapy emphasizing eccentric forearm flexor strengthening and progressive load adaptation.
- Topical or oral nonsteroidal anti-inflammatory medication for short-term symptom control.
- Corticosteroid injection at the flexor-pronator origin, used selectively. We use ultrasound guidance to keep the medication on the tendon and away from the ulnar nerve which sits directly behind the medial epicondyle.
- Platelet-rich plasma injection under ultrasound guidance is a reasonable consideration for chronic cases that have failed other measures and before surgery.
Surgical Options
Surgery is considered when symptoms persist beyond 6 to 12 months of structured conservative treatment, when imaging confirms established tendinopathy, and when the patient is significantly limited in work or sport.
Open Flexor-Pronator Release and Debridement
- Small incision over the medial epicondyle
- Identification and protection of the ulnar nerve, which lies in the cubital tunnel directly behind
- Removal of the diseased portion of the flexor-pronator tendon at its origin
- Decortication of the bone where the tendon attaches to stimulate healing
- Reattachment of the healthy tendon margins
- 30 to 45 minutes under regional or general anesthesia

Combined Procedure with Ulnar Nerve Decompression
When ulnar nerve compression coexists, ulnar nerve decompression at the cubital tunnel is performed in the same operation. This combination addresses both pain generators in one anesthetic and is associated with better overall outcomes than treating either condition alone in patients with both diagnoses.
Surgical success rates are 80 to 90 percent across published series. Workers' compensation cases and patients with chronic pain syndromes have somewhat lower success rates and require careful expectation setting.
Recovery Timeline
- Day 0: Procedure performed in 30 to 45 minutes. Sling applied. Discharge same day.
- Day 1 to 3: Sling rest. Light hand and wrist movement out of the sling. Bandage care per discharge instructions.
- Week 1: First follow-up. Sutures removed if not absorbable. Sling discontinued. Begin gentle elbow range of motion.
- Week 2 to 4: Daily home program of forearm range of motion. Driving resumed when off pain medication and able to grip the wheel.
- Week 4 to 8: Begin formal physical therapy. Eccentric forearm flexor strengthening, gradual return to daily activity.
- Week 8 to 12: Progressive return to repetitive tasks and the start of a coached return-to-sport protocol.
- Month 4 to 6: Full return to throwing, golf, or heavy manual work.
Returning to Work and Daily Activity
- Office or desk work: 1 to 2 weeks after surgery
- Light manual labor: 4 to 6 weeks
- Heavy manual labor: 8 to 12 weeks
- Throwing or golf: 3 to 6 months with a progressive coached protocol that addresses mechanics
- Driving: 1 to 2 weeks once sling is off and pain is controlled
Frequently Asked Questions
Is golfer's elbow only from playing golf?
No. Far fewer than half of patients with medial epicondylitis play golf. It is just as common in baseball pitchers, weightlifters, manual workers, and people who perform repetitive gripping. The name reflects the fact that golf swing mechanics load the medial elbow tendons heavily, but any repetitive flexion-gripping activity can produce the same problem.
Why do my fingers tingle along with my elbow pain?
The ulnar nerve runs in a tunnel directly behind the medial epicondyle. Roughly 20 to 30 percent of patients with chronic golfer's elbow develop coexisting ulnar nerve irritation that produces tingling in the ring and small fingers. We always evaluate both the tendon and the nerve. When both are involved, we can address both in the same operation.
Can I keep playing golf or throwing while it heals?
Continuing through pain reinforces the loading pattern that produced the tendinopathy and prolongs recovery. Most patients take a 4 to 8 week break, then return through a coached protocol that addresses swing or throwing mechanics. Your therapist or coach can help with the technical adjustments that prevent recurrence.
Are cortisone injections risky on the inner elbow?
Cortisone provides short-term relief but, like tennis elbow, multiple studies suggest no long-term benefit. The medial side carries an additional caution: the ulnar nerve sits directly behind the medial epicondyle, so injection accuracy matters. We use ultrasound guidance when injecting to keep the medication on the tendon and away from the nerve.
When is surgery the right answer for golfer's elbow?
Surgery is considered when pain has persisted longer than 6 to 12 months despite structured conservative care, AND imaging confirms tendinopathy, AND the patient is significantly limited in work or sport. Outcomes are 80 to 90 percent successful when the indication is correct. When ulnar nerve symptoms coexist, addressing both in the same operation improves overall results.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- Medial elbow pain that has lasted more than 6 weeks
- Pain that limits work, sport, or daily tasks
- Tingling or numbness in the ring and small fingers
- Failure of home conservative care including counterforce bracing
- Visible swelling, warmth, redness, or fever (these suggest infection or inflammatory arthritis and need prompt evaluation)
After surgery, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the incision
- Thick, yellow, or foul-smelling drainage
- Severe pain not controlled by prescribed medication
- Sudden new weakness or numbness in the hand or fingers
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Tennis Elbow (Lateral Epicondylitis): the same degenerative tendinopathy on the outer elbow at the extensor tendon origin. The opposite side of the same overuse pattern.
- Cubital Tunnel Syndrome: ulnar nerve compression at the elbow. Frequently coexists with golfer's elbow and is evaluated at every medial elbow visit.
- Hand and Wrist Arthritis: arthritis can refer pain into the forearm. Differentiated by joint-line tenderness and imaging.
- Carpal Tunnel Syndrome: median nerve compression at the wrist. Can coexist when the underlying problem is repetitive gripping.
- Trigger Finger: another tendon problem that often coexists with elbow tendinopathies in patients with repetitive gripping work.
From the Blog
- Tennis Elbow vs Golfer Elbow: lateral versus medial epicondylitis explained.
- When a Cortisone Injection Is the Right Choice: short-term relief for tendinopathy.
- Ergonomic Tips for Hand Pain: grip and tool changes that reduce flare-ups.
Watch: Medial elbow pain education
Short videos from Dr. Loredo's YouTube and Facebook channels.