Tennis elbow, or lateral epicondylitis, is a degenerative tendinopathy of the common extensor tendon at the outside of the elbow. The hallmark presentation is pain at the bony bump on the outer elbow that worsens with gripping, lifting with the palm down, or shaking hands. Most cases improve with activity modification, counterforce bracing, targeted physical therapy, and time. When symptoms persist beyond 6 to 12 months despite conservative care, options include corticosteroid injection, platelet-rich plasma injection, or surgical release of the affected tendon origin.
The Anatomy of the Lateral Elbow
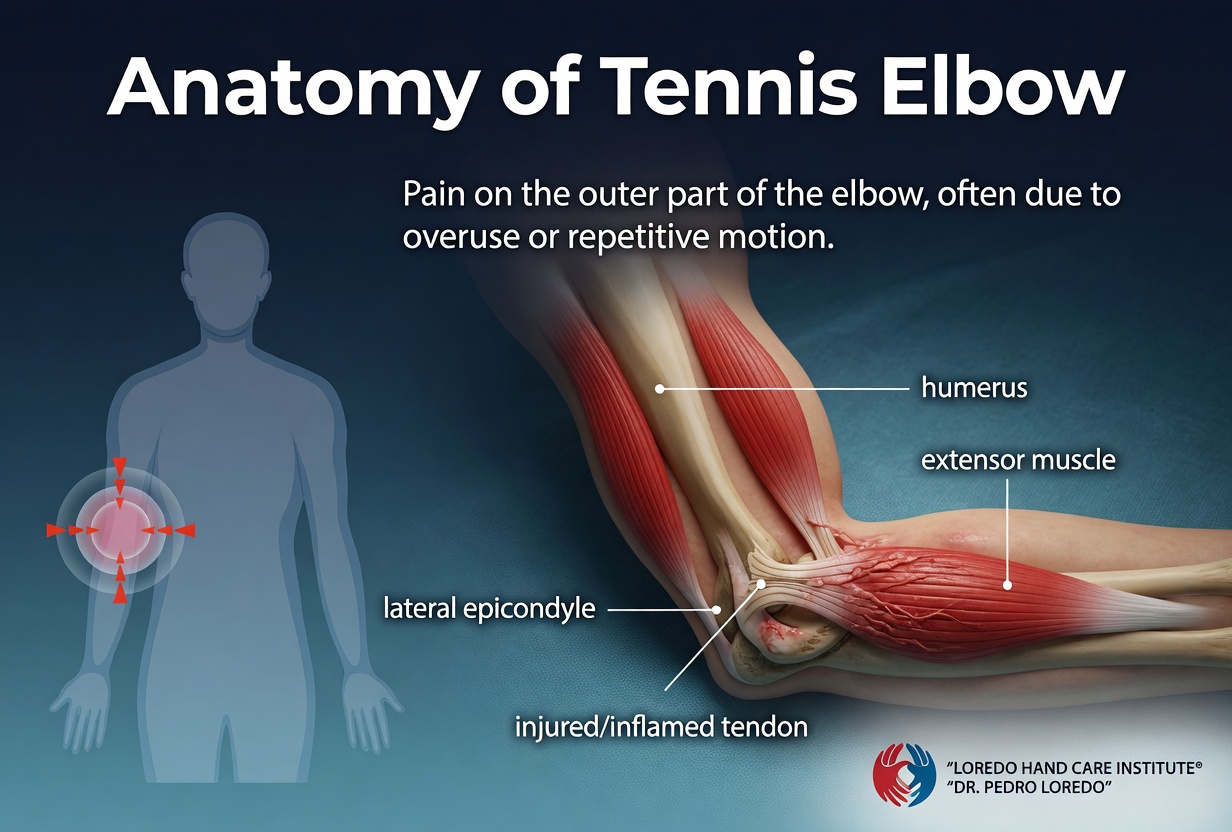
The lateral epicondyle is the small bony bump on the outside of the elbow at the end of the humerus. It is the shared origin point for the muscles that extend the wrist and fingers, including the extensor carpi radialis brevis (ECRB), the extensor carpi radialis longus, the extensor digitorum, and the extensor carpi ulnaris. The ECRB is the most commonly affected tendon in tennis elbow. Its tendon attaches to the lateral epicondyle and runs distally across the forearm to the base of the third metacarpal.
The pathology is angiofibroblastic degeneration of the deep surface of the ECRB tendon at its attachment to bone. Microscopic tears, disorganized collagen, and abnormal blood vessel ingrowth replace the normally dense, parallel tendon structure. This is why the historical term "epicondylitis" is misleading: there is little acute inflammation in established cases. Recovery is driven by load management and targeted strengthening, not by anti-inflammatories.
Clinical coding: ICD-10 M77.10 (lateral epicondylitis, unspecified). SNOMED CT 202855006.
Causes and Risk Factors
Tennis elbow is an overuse condition. The tendon is loaded faster than it can adapt and remodel. Common contributors:
- Repetitive forearm extension and forceful gripping at work or in sport
- Racquet sports including tennis, pickleball, racquetball, and squash, particularly with heavy racquets, tight strings, or backhand stroke errors
- Manual occupations such as carpentry, plumbing, electrical work, and assembly line work
- Sustained computer mouse use over hours with a poorly fitted workstation
- Age 35 to 55 when tendon biology begins to shift
- Smoking and diabetes, which impair tendon healing and alter collagen quality
- Sudden increases in training intensity without progressive load adaptation
Despite the name, fewer than 10 percent of patients with tennis elbow actually play tennis.
Symptoms and Warning Signs

- Pain at the bony bump on the outside of the elbow
- Pain that radiates down the back of the forearm toward the wrist
- Pain on shaking hands, lifting a coffee mug, or turning a doorknob
- Pain reproduced when lifting an object with the palm facing down
- Weakness of grip, often more painful than truly weak in early cases
- Tenderness on direct pressure 1 to 2 cm distal and slightly anterior to the lateral epicondyle
- Symptoms that worsen gradually over weeks to months without a single clear injury
- Morning stiffness in the elbow that loosens with light activity
How the Diagnosis Is Made
Tennis elbow is a clinical diagnosis. History and a focused examination are sufficient in most cases. Dr. Loredo performs three standard provocative tests:
- Cozen's test (resisted wrist extension): with the elbow extended and the forearm pronated, the patient extends the wrist against the examiner's resistance. Reproduction of pain at the lateral epicondyle is positive. This is the most commonly used bedside test.
- Mill's test: the examiner passively flexes the patient's wrist with the elbow extended and forearm pronated. The maneuver stretches the ECRB tendon and reproduces lateral epicondylar pain in tennis elbow.
- Maudsley's test (resisted middle finger extension): with the elbow extended and forearm pronated, the patient extends the middle finger against resistance. Reproduced pain at the lateral epicondyle implicates the ECRB specifically because that tendon shares attachment with the middle finger extensor.
Imaging is not always required. X-ray rules out joint pathology, calcification, or arthritis. MRI or ultrasound confirms tendinopathy and grades severity when symptoms persist or surgery is contemplated. Ultrasound is useful at the bedside and shows tendon thickening, hypoechoic regions, and abnormal blood vessel ingrowth on Doppler. EMG is ordered when radial tunnel syndrome is part of the differential.
Non-Surgical Treatment Options
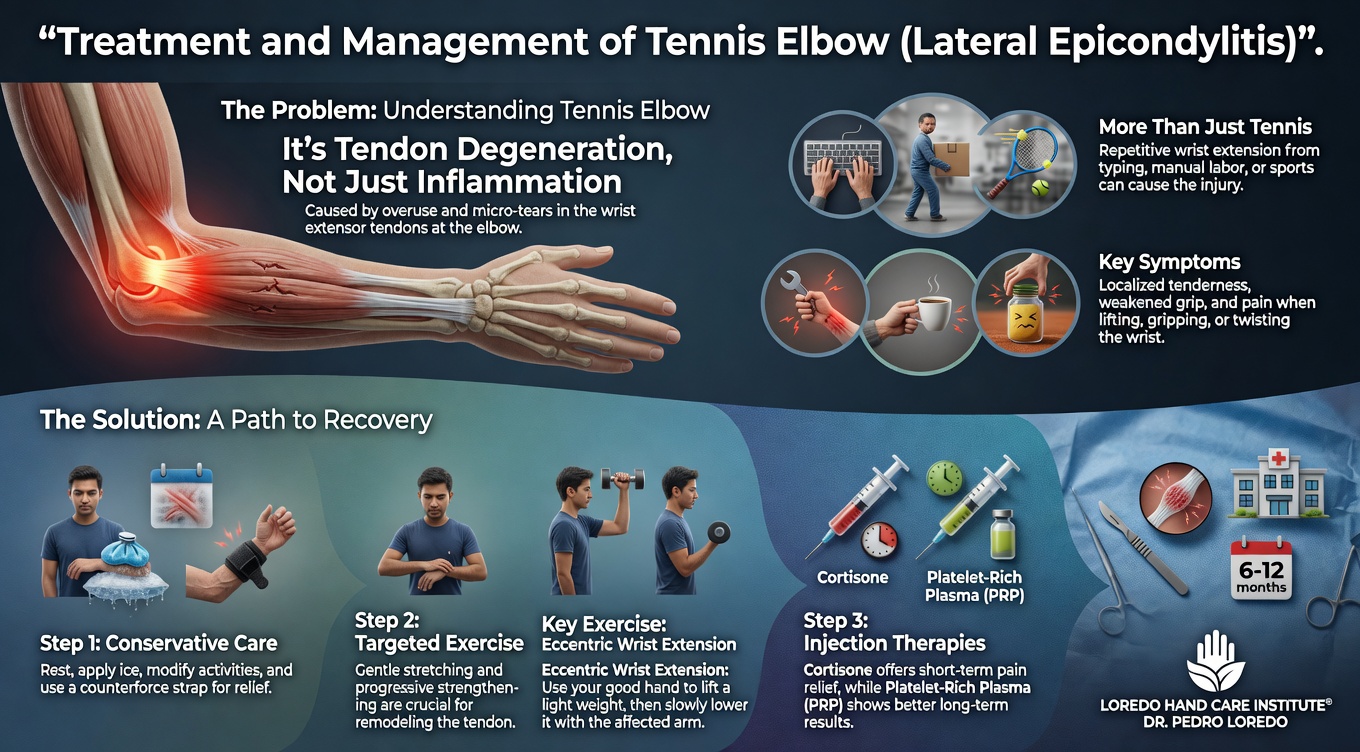
Roughly 80 percent of cases resolve within 6 to 12 months with consistent conservative care. Treatment escalates from least to most invasive based on response.
- Activity modification: avoid the repetitive gripping and palm-down lifting that aggravates the tendon. Modify backhand mechanics, swap a heavier racquet for a lighter one, or rotate work tasks where possible.
- Counterforce brace: a forearm strap worn 1 to 2 inches distal to the lateral epicondyle redistributes load away from the painful tendon origin. Worn during aggravating activities only.
- Wrist extension splint at night reduces ECRB tension during sleep.
- Targeted physical therapy with a hand therapist. The cornerstone is eccentric forearm extensor strengthening. The Tyler Twist with a flexible bar is one validated protocol.
- Topical or oral nonsteroidal anti-inflammatory medication for early symptomatic relief.
- Corticosteroid injection gives short-term pain relief but studies suggest long-term outcomes are no better, and may be worse, than activity modification alone. Used selectively when disabling pain prevents participation in therapy.
- Platelet-rich plasma injection under ultrasound guidance has emerging evidence in chronic cases that have failed conservative care. Reasonable to consider before surgery.
Surgical Options
Surgery is considered when symptoms persist beyond 6 to 12 months of structured conservative treatment, when imaging shows established tendinopathy, and when the patient is significantly limited in work, sport, or daily life.
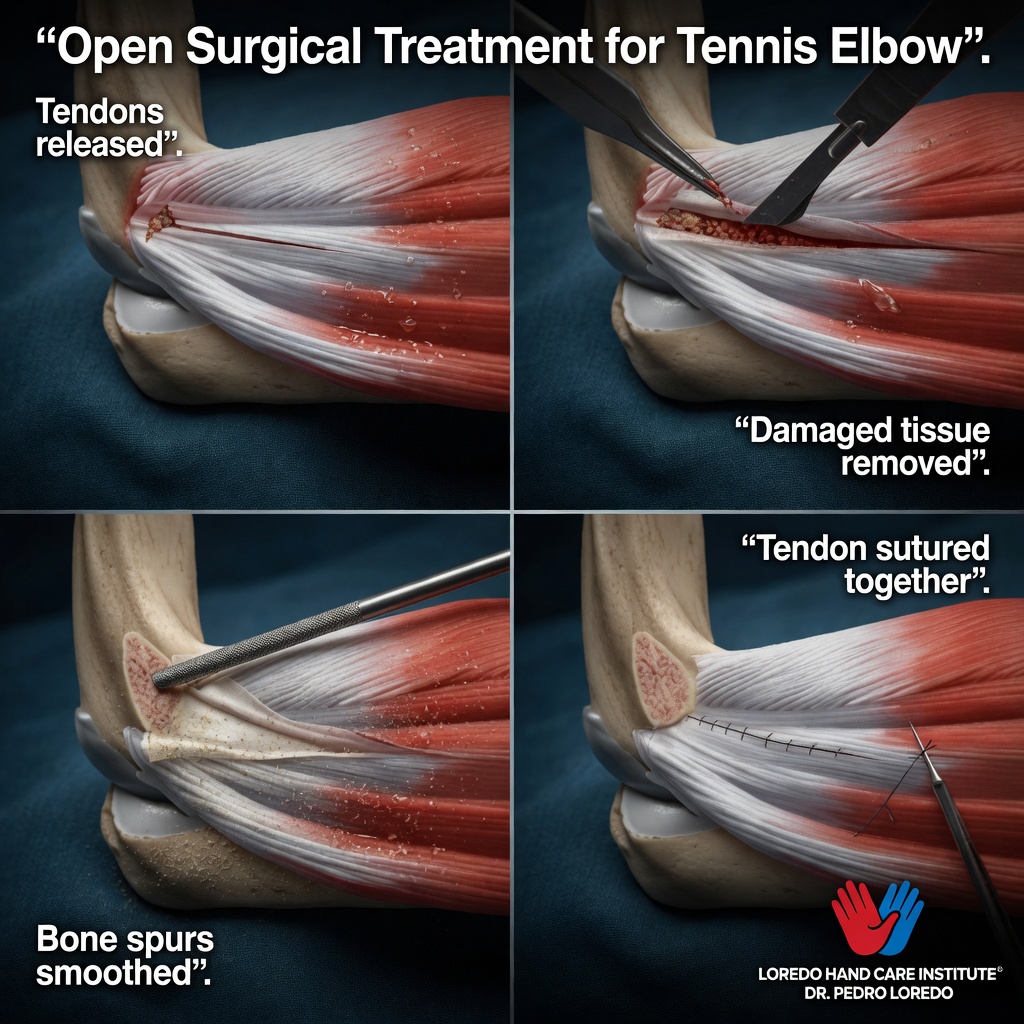
Open ECRB Release and Debridement
- Small incision over the lateral epicondyle
- Direct exposure and removal of the diseased portion of the ECRB tendon
- Decortication of the bone where the tendon attaches to stimulate a healing response
- Reattachment of the healthy tendon margins
- Procedure takes 30 to 45 minutes under local or regional anesthesia
- Small dressing and a sling for the first few days

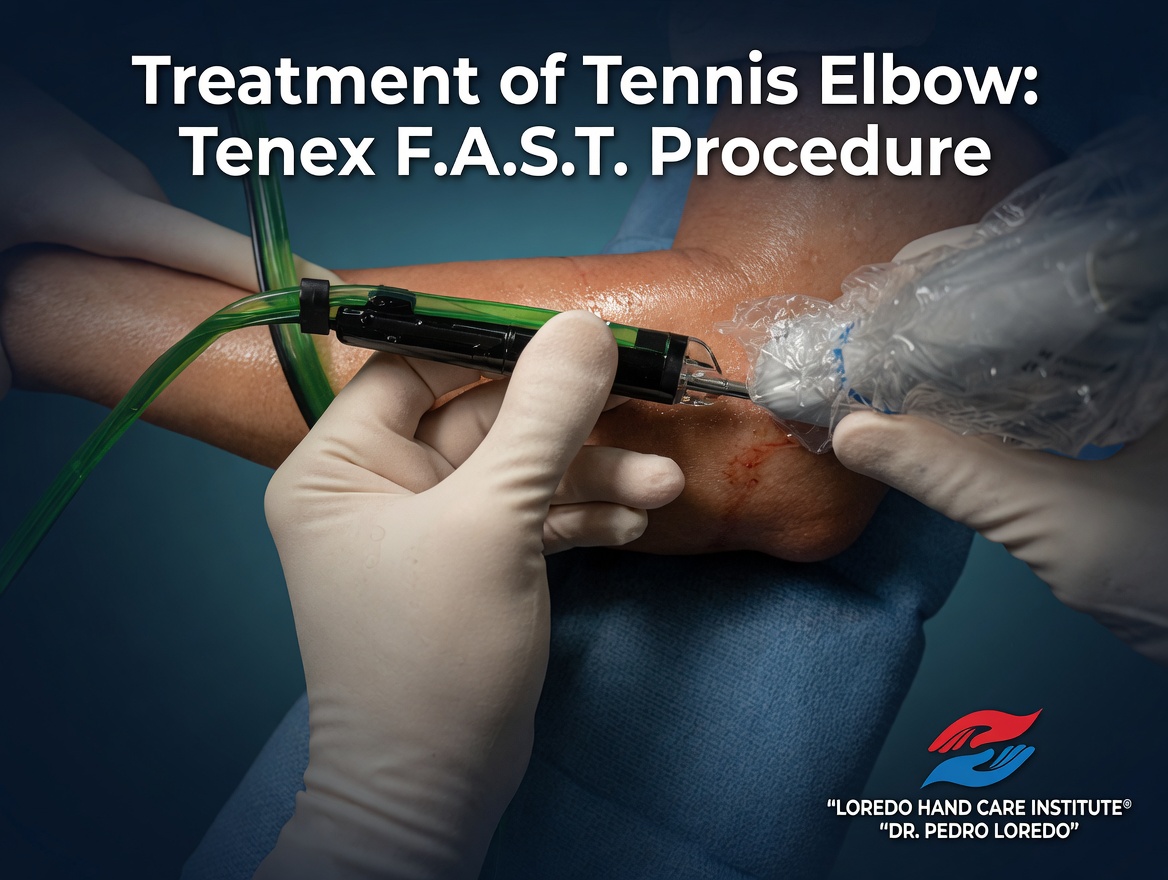
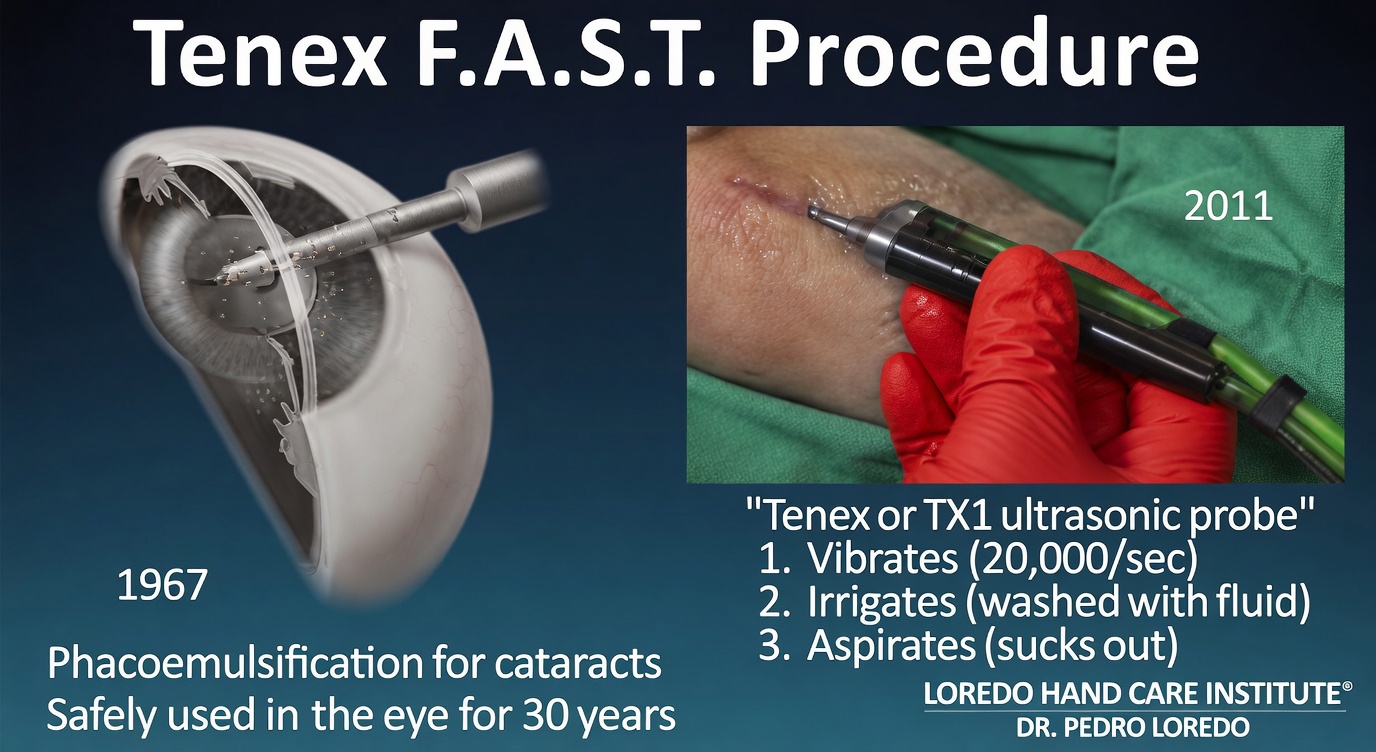
Tenex FAST Percutaneous Tenotomy
Tenex FAST (Focused Aspiration of Scar Tissue) is an FDA-cleared, ultrasound-guided procedure that targets the diseased ECRB tendon through a single needle entry rather than a surgical incision. A specialized handpiece uses ultrasonic energy to break up and aspirate the angiofibroblastic tissue at the tendon origin, leaving the healthy tendon undisturbed.
- Performed in the office or outpatient surgery center under local anesthesia
- No skin incision and no sutures; the small needle entry is closed with an adhesive strip
- Procedure takes 15 to 20 minutes; most patients drive themselves home
- Return to light daily activity is typically faster than open release
- Published outcomes are comparable to open ECRB release at one to two years in appropriately selected patients
Surgical success rates are 85 to 95 percent across published series. Recurrence after surgery is uncommon. Workers' compensation cases and patients with chronic pain syndromes have somewhat lower success rates and require careful expectation setting before surgery is scheduled.
Recovery Timeline
- Day 0: Procedure performed in 30 to 45 minutes under local or regional anesthesia. Sling applied. Discharge same day.
- Day 1 to 3: Sling rest. Light hand and wrist movement out of the sling several times per day. Bandage care per discharge instructions.
- Week 1: First follow-up. Sutures removed if not absorbable. Sling discontinued. Begin gentle elbow range of motion.
- Week 2 to 4: Daily home program of forearm range of motion. Driving resumed when off pain medication and able to grip the wheel without sharp pain. Light typing and writing.
- Week 4 to 8: Begin formal physical therapy. Eccentric forearm extensor strengthening, gradual return to activities of daily living.
- Week 8 to 12: Progressive return to repetitive tasks at work. Manual labor and racquet sports begin in this window.
- Month 4 to 6: Full return to sport. Tendon remodeling continues for up to a year.
Returning to Work and Daily Activity
- Office or desk work: 1 to 2 weeks after surgery
- Light manual labor: 4 to 6 weeks
- Heavy manual labor (carpentry, plumbing, lifting more than 25 lbs repeatedly): 8 to 12 weeks
- Racquet sports: 3 to 6 months with progressive return through a coached protocol that addresses backhand mechanics
- Driving: 1 to 2 weeks once sling is off and pain is well controlled
Frequently Asked Questions
Do I really have to stop playing tennis?
Not forever, but yes during the acute phase. Continuing to play through pain reinforces the same loading pattern that caused the tendinopathy and prolongs recovery. Most patients do best with a 4 to 8 week pause from racquet sports while tendons heal, then a structured return that addresses backhand mechanics, racquet weight, and string tension. A coach or physical therapist familiar with overuse injuries can help avoid the pattern that produced the injury.
How long does tennis elbow take to heal?
About 80 percent of cases resolve within 6 to 12 months of consistent conservative care. Some cases improve in weeks. Chronic cases that have lasted more than a year, or cases with significant tendon thickening on imaging, may not fully resolve without targeted intervention. Surgery is considered when conservative treatment has had a fair trial and symptoms continue to limit function.
Are cortisone shots safe for tennis elbow?
Cortisone provides short-term pain relief, often dramatic, but multiple high-quality studies suggest that long-term outcomes are no better, and may be worse, than activity modification alone. We use cortisone selectively, usually a single injection in patients whose pain is severe enough to prevent participation in therapy. Repeated injections at the same site can weaken the tendon and are avoided.
What is PRP and is it worth it?
Platelet-rich plasma is concentrated platelets prepared from your own blood and injected under ultrasound guidance into the diseased tendon. Growth factors stimulate collagen repair where chronic tendinopathy has stalled. Evidence in lateral epicondylitis is more favorable than for cortisone in chronic cases. PRP is reasonable to consider after at least 3 to 6 months of failed conservative care and before surgery. Most insurance plans do not cover PRP and patients pay out of pocket.
How do I know if I need surgery for tennis elbow?
Surgery is indicated when pain has persisted longer than 6 to 12 months despite a structured course of activity modification, bracing, therapy, and at least one injection trial when appropriate, AND imaging confirms established tendinopathy, AND the patient is significantly limited in work, sport, or daily life. Surgery is not the first answer for tennis elbow. When the indication is right, results are excellent in 85 to 95 percent of cases.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- Lateral elbow pain that has lasted more than 6 weeks
- Pain that limits work, sport, or daily tasks like lifting a coffee mug
- Failure of home conservative care including counterforce bracing
- Visible swelling, warmth, redness, or fever (these suggest infection or inflammatory arthritis and need prompt evaluation)
After surgery, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the incision
- Thick, yellow, or foul-smelling drainage from the wound
- Severe pain that is not controlled by prescribed medication
- Sudden new weakness or numbness in the hand or fingers
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Golfer's Elbow (Medial Epicondylitis): the same degenerative tendinopathy on the inner elbow at the flexor-pronator tendon origin. Often confused with tennis elbow but on the opposite side of the elbow.
- Cubital Tunnel Syndrome: ulnar nerve compression at the elbow. Can coexist with golfer's elbow on the medial side and occasionally produces vague elbow pain.
- Hand and Wrist Arthritis: arthritis can cause referred pain into the forearm. Differentiate by joint-line tenderness and imaging.
- De Quervain's Tendonitis: another tendinopathy, located at the wrist rather than the elbow. Both conditions respond to load reduction and eccentric strengthening principles.
- Carpal Tunnel Syndrome: forearm pain occasionally radiates from carpal tunnel and can be confused with elbow pathology in atypical cases.
From the Blog
- Tennis Elbow vs Golfer Elbow: lateral versus medial epicondylitis explained.
- When a Cortisone Injection Is the Right Choice: short-term relief for tendinopathy.
- Ergonomic Tips for Hand Pain: wrist position and tool grip changes.
Watch: Lateral elbow pain education
Short videos from Dr. Loredo's YouTube and Facebook channels.