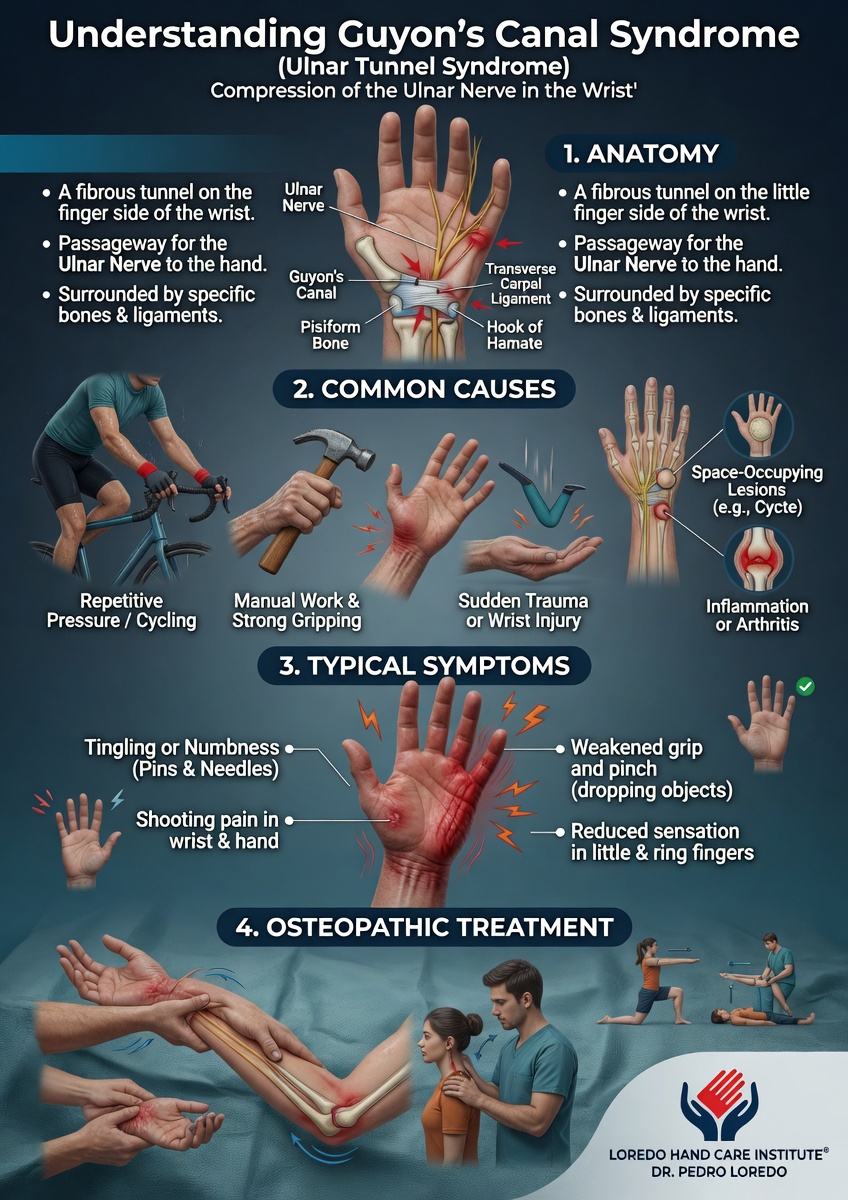
Guyon's canal syndrome is compression of the ulnar nerve as it passes through the wrist between the pisiform bone and the hook of the hamate. Symptoms include numbness and tingling in the ring and small fingers, weak grip, and in advanced cases visible thinning of the small muscles between the thumb and index finger. The condition is most commonly seen in long-distance cyclists, jackhammer operators, and others with sustained pressure on the ulnar side of the palm. Treatment ranges from padded gloves and ergonomic modification to surgical decompression of the canal, sometimes combined with excision of an underlying ganglion cyst.
The Anatomy of Guyon's Canal
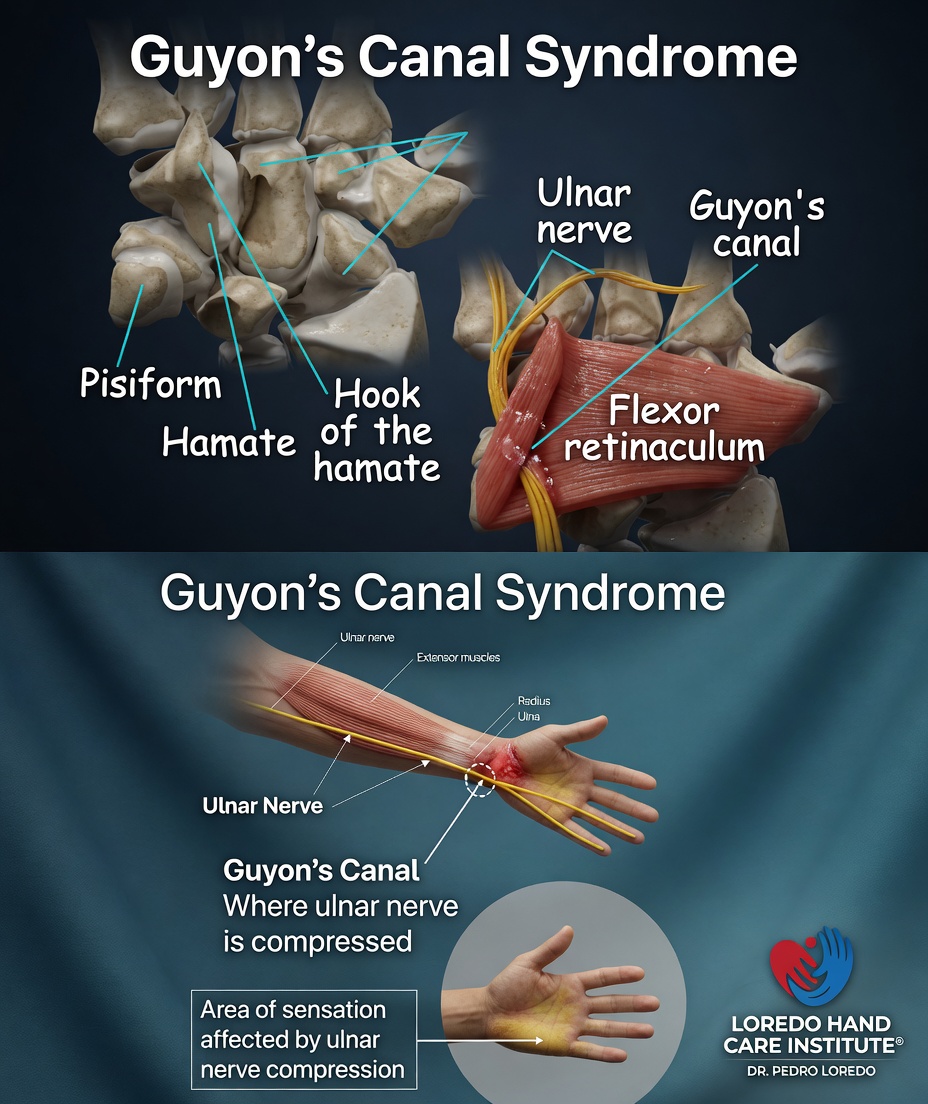
Guyon's canal is a narrow tunnel on the palm side of the wrist, just inside (medial to) the carpal tunnel. The floor of the canal is the transverse carpal ligament. The roof is the volar carpal ligament and the palmaris brevis muscle. The two bony walls are the pisiform on the ulnar (small finger) side and the hook of the hamate on the radial (thumb) side.
The ulnar nerve and ulnar artery enter the canal together at the wrist. Inside the canal the ulnar nerve splits into two branches: a superficial sensory branch that supplies feeling to the small finger and the ulnar half of the ring finger, and a deep motor branch that powers most of the intrinsic hand muscles, including the hypothenar muscles, the interosseous muscles between the metacarpals, and the adductor pollicis at the base of the thumb. The deep motor branch curves around the hook of the hamate after it leaves the canal, which is why a fracture of the hook of the hamate can selectively damage the motor branch and produce intrinsic weakness without sensory loss.
One important anatomic detail separates Guyon's canal from cubital tunnel syndrome at the elbow: the dorsal sensory branch of the ulnar nerve, which supplies sensation to the back of the ulnar side of the hand, leaves the main ulnar nerve in the forearm before it reaches Guyon's canal. Compression at Guyon's canal therefore spares dorsal hand sensation. Compression at the elbow produces numbness on both the palmar and dorsal sides. The presence or absence of dorsal hand numbness is one of the most useful bedside findings for telling the two conditions apart.
Clinical coding: ICD-10 G56.21 (lesion of ulnar nerve, upper limb). SNOMED CT 85305003.
Causes and Risk Factors
- Long-distance cycling with prolonged pressure on the ulnar palm at the handlebars (the classic "handlebar palsy")
- Vibration tool use including jackhammers, grinders, and pneumatic equipment
- Ganglion cyst within or near the canal: the most common identifiable structural cause
- Hook of hamate fracture, often after a missed swing while gripping a club, bat, or racquet
- Prolonged pressure on the ulnar palm from work tools, walkers, crutches, or wheelchair use
- Anatomic anomalies such as an accessory muscle in the canal
- Repetitive trauma from manual occupations
- Diabetes, which makes nerves more vulnerable to compression at any site
Symptoms and Warning Signs
- Numbness or tingling in the small finger and the ulnar half of the ring finger (palmar surface only)
- Normal sensation on the back of the hand (a key feature)
- Weak grip and difficulty with pinch tasks
- Weakness when spreading the fingers apart or bringing them together
- Difficulty with fine motor tasks like buttoning shirts, picking up small objects, or typing
- Visible thinning of the muscle between the thumb and index finger in advanced cases (first dorsal interosseous wasting)
- Mild claw deformity of the ring and small fingers in severe long-standing cases
- Symptoms reproduced or worsened by sustained gripping or pressure on the ulnar palm
How the Diagnosis Is Made
The evaluation begins with a focused history (cycling, vibration tool use, prior hook of hamate injury) and a careful examination that maps the sensory loss and tests the strength of the small hand muscles. Dr. Loredo performs several standard tests:
- Tinel's sign at Guyon's canal: tapping over the canal at the base of the hypothenar eminence reproduces tingling into the ring and small fingers.
- Froment's sign: the patient pinches a piece of paper between the thumb and index finger. With weakness of the adductor pollicis (deep motor branch), the patient compensates by flexing the thumb interphalangeal joint, a sign of intrinsic weakness.
- Palmar versus dorsal sensory split test: sensation is checked on both sides of the hand. Normal dorsal sensation with abnormal palmar sensation localizes the lesion to Guyon's canal rather than the elbow.
- Wartenberg's sign: the small finger drifts into abduction at rest in advanced cases, reflecting weakness of the third palmar interosseous muscle.
- Crossed-finger test: inability to cross the index finger over the middle finger reflects weakness of the second palmar interosseous.
Confirmatory testing includes electrodiagnostic studies (EMG and nerve conduction studies) that localize and grade the compression. Ultrasound or MRI of the wrist is used selectively to look for a ganglion cyst, an accessory muscle, or other space-occupying lesion within the canal. X-ray of the wrist with a carpal tunnel view is appropriate when a hook of hamate fracture is suspected after a swing injury.
Non-Surgical Treatment Options
- Padded gloves and gel handlebar tape for cyclists. Frequent changes in hand position during long rides distribute load away from any one pressure point.
- Anti-vibration gloves for workers using power tools.
- Ergonomic modification of work tasks, walker handles, or wheelchair controls to remove sustained pressure on the ulnar palm.
- Wrist splinting in a neutral position, particularly at night, to reduce wrist motion that aggravates the canal.
- Activity modification: reduce or rotate aggravating tasks for several weeks.
- Targeted hand therapy for nerve and tendon gliding exercises and intrinsic muscle strengthening.
- Topical or oral nonsteroidal anti-inflammatory medication for short-term symptom relief.
Most cases related to cycling or external pressure resolve fully with consistent conservative care over 6 to 12 weeks. Cases caused by a ganglion cyst or hook of hamate fracture typically require structural treatment.
Surgical Options
Surgery is considered when conservative care has failed for several months, when imaging shows a structural cause (ganglion cyst, accessory muscle, fracture), or when there is significant motor weakness or muscle wasting that warrants prompt decompression.
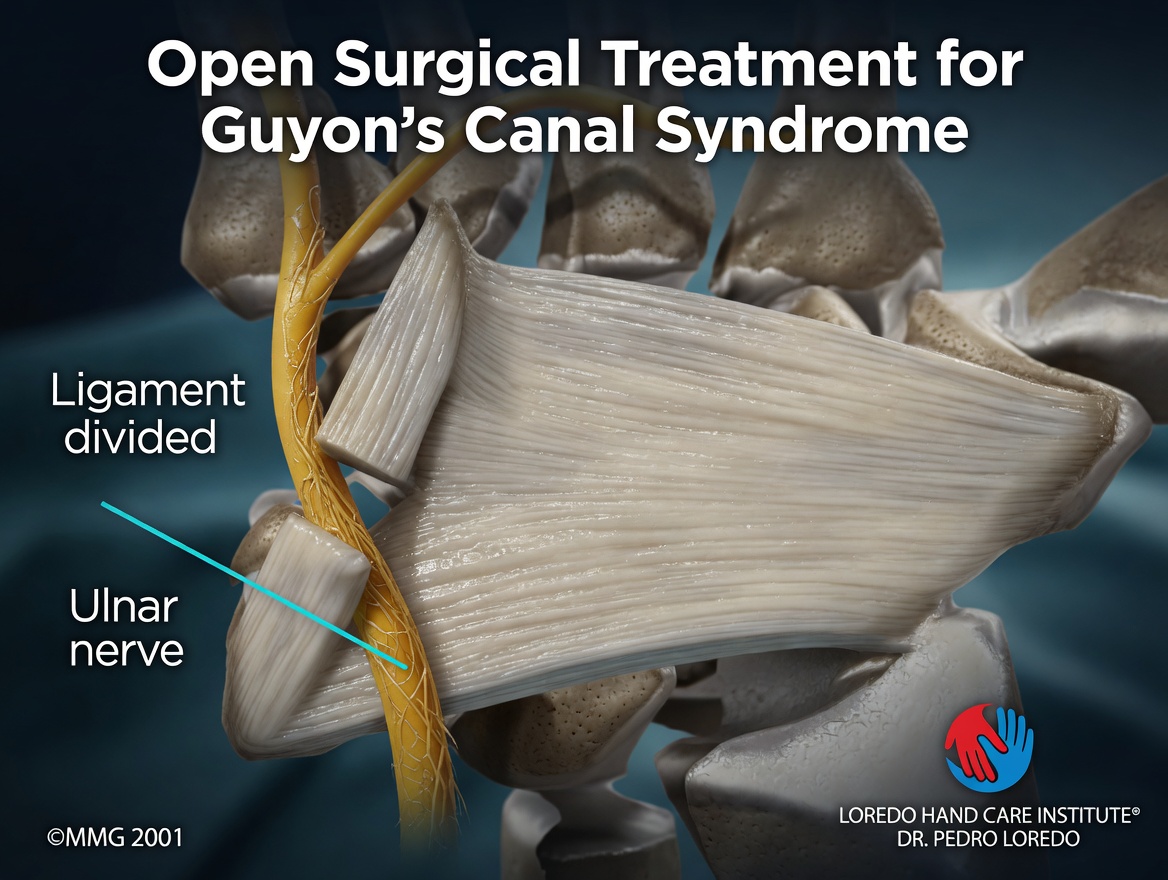
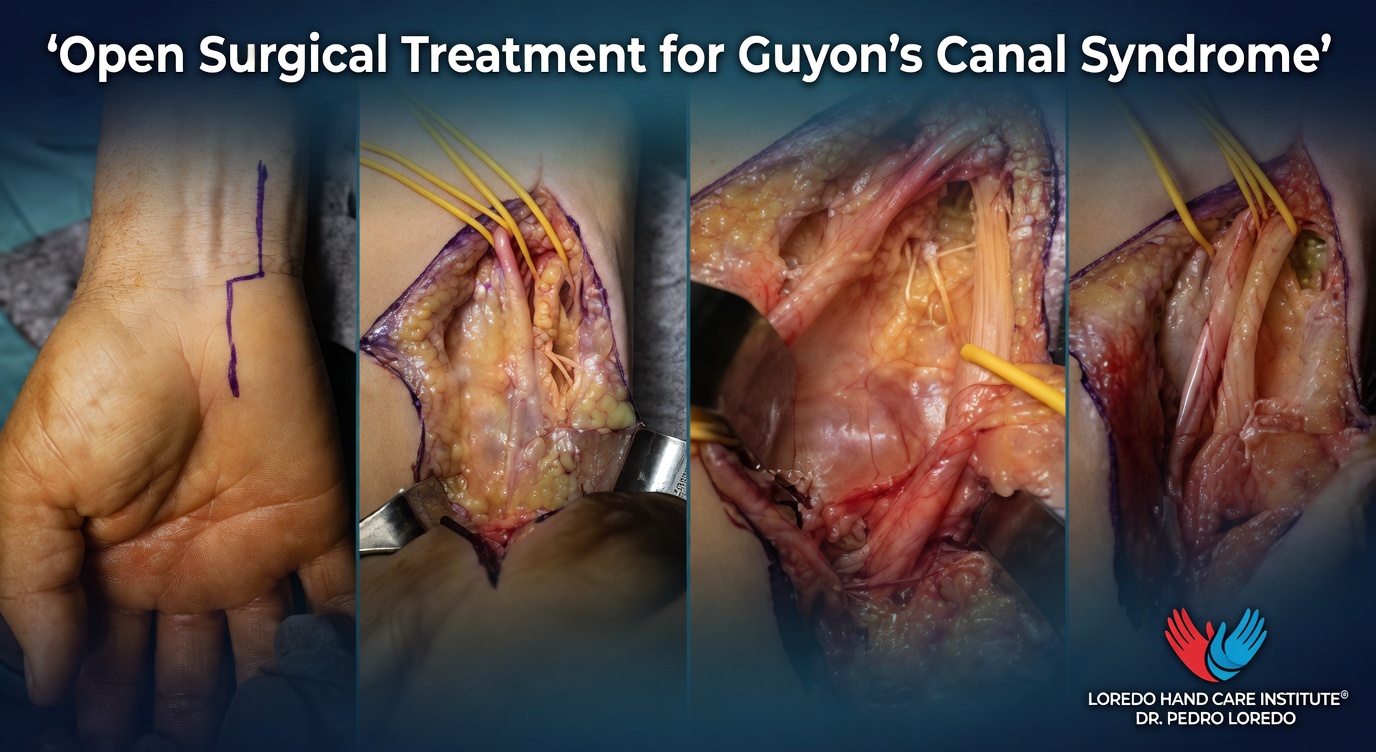
Ulnar Nerve Decompression at Guyon's Canal
- Small incision over the volar ulnar wrist
- Release of the volar carpal ligament that forms the roof of the canal
- Identification and protection of the ulnar nerve and artery
- Division of any tight fascial bands compressing the nerve in zones 1, 2, or 3 of the canal
- Excision of a ganglion cyst or accessory muscle if present
- Procedure takes 30 to 45 minutes under local or regional anesthesia
- Soft dressing and removable splint for the first week
Combined Carpal Tunnel and Guyon's Canal Release
Patients with both conditions can have both tunnels released in the same operation through separate small incisions. Combined surgery is well tolerated and avoids two anesthetics.
Recovery Timeline
- Day 0: Procedure performed in 30 to 45 minutes. Removable splint applied. Discharge same day.
- Day 1 to 7: Light hand and finger motion several times per day. Bandage care per discharge instructions.
- Week 1 to 2: First follow-up. Sutures removed if not absorbable. Begin gentle wrist range of motion.
- Week 2 to 6: Progressive grip and pinch strengthening. Hand therapy as needed for nerve gliding exercises.
- Week 6 to 12: Sensory recovery progressing. Most patients return to manual labor and athletic activity in this window.
- Month 3 to 12: Motor recovery continues. Severe cases with muscle wasting before surgery may have ongoing improvement for up to a year, though some residual weakness may remain.
Returning to Work and Daily Activity
- Office or desk work: 1 to 2 weeks after surgery
- Light manual labor: 4 to 6 weeks
- Heavy manual labor and vibration tool use: 8 to 12 weeks
- Cycling: stationary bike at 4 weeks; outdoor cycling with padded gloves and gel tape at 6 to 8 weeks
- Driving: 1 to 2 weeks, once off pain medication and able to grip the wheel comfortably
Frequently Asked Questions
How is Guyon's canal syndrome different from cubital tunnel syndrome?
Both conditions affect the ulnar nerve, but at different levels. Cubital tunnel is compression at the elbow and produces numbness on both the palmar and dorsal sides of the ring and small fingers, plus the dorsal hand. Guyon's canal compression is at the wrist and spares the dorsal sensation entirely because the dorsal sensory branch leaves the ulnar nerve before it enters Guyon's canal. The presence or absence of dorsal hand numbness is one of the most useful bedside findings for telling them apart.
Why is this called handlebar palsy?
Cyclists who grip drop handlebars for long rides put sustained pressure on the ulnar side of the palm directly over Guyon's canal. The result is compression of the ulnar nerve at the wrist with numbness in the ring and small fingers and weakness of the small hand muscles. Padded gloves, gel handlebar tape, and changes in hand position during long rides usually resolve the problem before it becomes chronic.
What causes Guyon's canal syndrome besides cycling?
A ganglion cyst within or near the canal is the most common identifiable structural cause. Other causes include repetitive jackhammer or vibration tool use, trauma from a fracture of the hook of the hamate, and rarely a benign mass. In many patients no specific cause is identified and the symptoms are attributed to cumulative pressure or microtrauma.
Will my hand strength come back after surgery?
Sensory recovery after Guyon's canal decompression is generally good and usually progresses over 6 to 12 weeks. Motor recovery is more variable and depends on how long the nerve was compressed and how severe the muscle wasting was before surgery. Mild to moderate cases typically recover near-normal strength. Severe long-standing cases with visible muscle thinning may have permanent weakness even after a successful decompression. Earlier treatment leads to more complete recovery.
Is the surgery for Guyon's canal syndrome the same as carpal tunnel surgery?
No. Although both involve releasing a tunnel at the wrist, the carpal tunnel and Guyon's canal are separate anatomic structures, and the surgical approach, dissection, and post-operative recovery differ. Some patients with severe nerve compression have both conditions and benefit from a combined operation. Each tunnel is opened through its own approach, and the recovery follows the same general timeline.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- Ring and small finger numbness or tingling that persists more than a few weeks
- Weakness in grip, pinch, or finger spread
- Visible thinning of the muscle between the thumb and index finger
- Symptoms after a fall, hard swing with a club or bat, or direct blow to the palm
- Failure to improve with padded gloves and ergonomic changes after several weeks
After surgery, call the office promptly if you experience:
- Fever over 101°F, chills, or flu-like symptoms
- Expanding redness or warmth around the incision
- Thick, yellow, or foul-smelling drainage
- Severe pain not controlled by prescribed medication
- New numbness that worsens rather than improves, or color changes in the hand
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Cubital Tunnel Syndrome: ulnar nerve compression at the elbow. The most important alternative diagnosis. Differentiated by the presence of dorsal hand numbness (cubital tunnel) versus its absence (Guyon's canal).
- Carpal Tunnel Syndrome: median nerve compression at the wrist. The two tunnels sit side by side and both conditions can coexist, particularly in patients with diabetes.
- Hand and Finger Fractures: a hook of hamate fracture is a recognized cause of selective ulnar motor weakness and is suspected when symptoms follow a swing injury with a club, bat, or racquet.
- Hand and Wrist Arthritis: arthritis-related synovitis can occasionally compress the ulnar nerve at the wrist, particularly in rheumatoid disease.
- Trigger Finger: a different palmar problem that occasionally coexists with nerve compression syndromes in patients with diabetes or repetitive gripping work.
From the Blog
- The Ulnar Nerve and Why It Matters: full anatomy and the three main compression sites.
- Is It Cubital Tunnel or a Pinched Neck Nerve?: distinguishing nerve compression sites.
Watch: Ulnar nerve at the wrist education
Short videos from Dr. Loredo's YouTube and Facebook channels.