Pregnancy and postpartum hand pain is common and usually treatable without surgery. Two patterns dominate. Pregnancy-related carpal tunnel syndrome appears in the second and third trimesters from fluid retention and hormonal changes that compress the median nerve at the wrist. Symptoms include hand numbness, tingling, and night pain. Postpartum De Quervain's tenosynovitis ("mommy thumb") appears 4 to 6 weeks after delivery from the repetitive lifting that infant care requires, producing thumb-side wrist pain that worsens with lifting the baby. Trigger finger and general arthralgias also appear in this period. Treatment is staged: pregnancy-safe options first (splinting, hand therapy, ergonomic modification, ice, acetaminophen), with selective corticosteroid injection or surgery reserved for severe or persistent symptoms. Most pregnancy-related hand conditions resolve within 2 to 6 months of delivery.
Why Pregnancy Affects the Hands
Pregnancy produces several changes that predispose the hands and wrists to specific conditions. Fluid retention increases tissue volume in narrow anatomic tunnels like the carpal tunnel. Hormonal changes (relaxin, estrogen, and progesterone) increase ligament laxity and tendon swelling throughout the body. Weight gain shifts posture and grip patterns. The pregnant body holds approximately 6 to 8 extra liters of total body water by the third trimester, and even modest amounts of that fluid in the carpal tunnel can compress the median nerve.
Postpartum, the dominant change shifts. Fluid retention resolves over 4 to 8 weeks. Hormonal shifts continue, particularly during breastfeeding. The repetitive load of infant care begins: lifting a 7 to 10 pound baby out of a bassinet 20 to 30 times a day, holding the head with the thumb extended, supporting the breastfeeding latch, and maneuvering car seats. The thumb-side wrist tendons of the first dorsal compartment are particularly vulnerable to this loading pattern, which is why postpartum De Quervain's is so common.
Clinical coding: ICD-10 O26.89 (other specified pregnancy-related conditions), G56.0 (carpal tunnel), M65.4 (De Quervain's), M65.3 (trigger finger). SNOMED CT 57406009 (CTS).
Common Hand Conditions in Pregnancy and Postpartum
Pregnancy-Related Carpal Tunnel Syndrome
Up to half of pregnant women develop some carpal tunnel symptoms in the second or third trimester. Numbness, tingling, and weakness in the thumb, index, middle, and half of the ring finger are typical. Night symptoms are common as the patient lies down and fluid redistributes into the wrists. Most cases are mild and resolve within 4 to 12 weeks of delivery as fluid retention decreases.

Postpartum De Quervain's Tenosynovitis
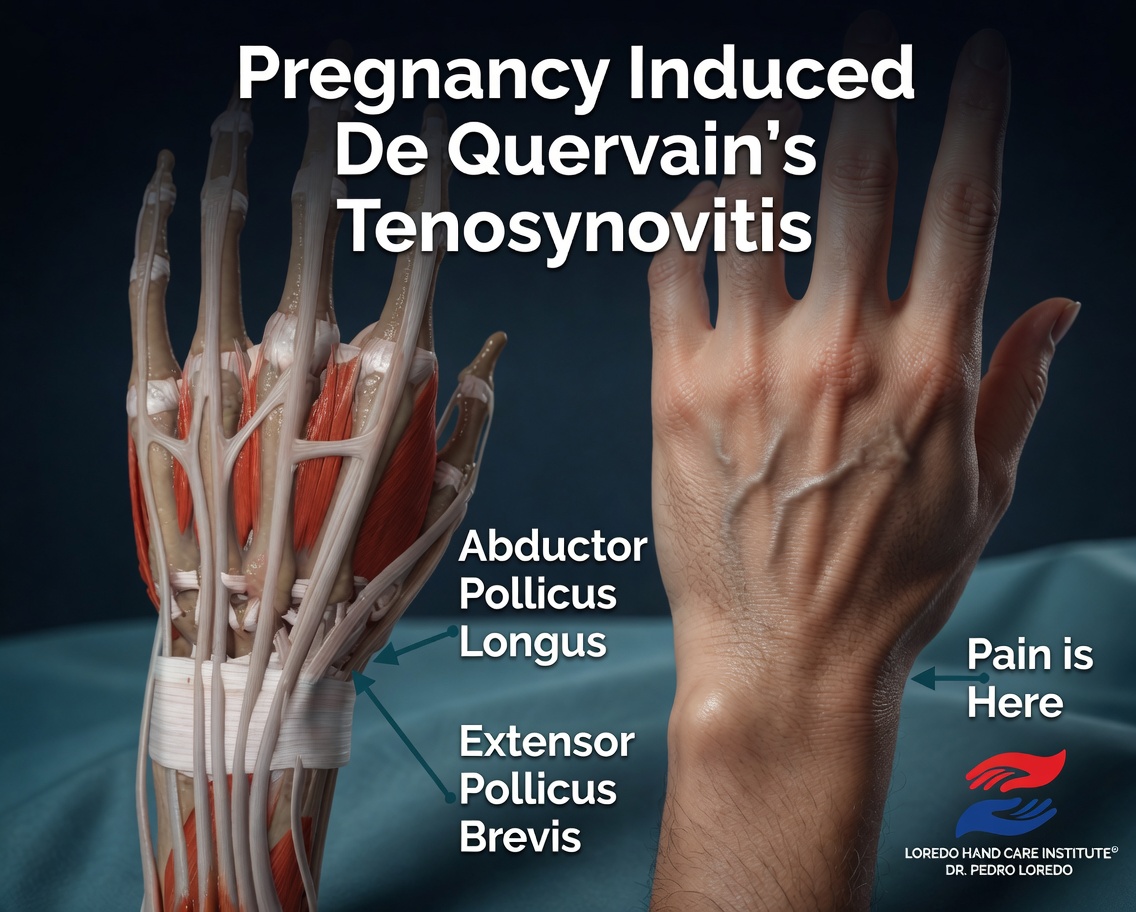
Often called mommy thumb. The abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons of the first dorsal compartment become inflamed from repetitive infant lifting and breastfeeding positions. Pain at the thumb side of the wrist that worsens with thumb motion or with ulnar deviation of the wrist (Finkelstein test) is the classic presentation. Symptoms typically begin 4 to 6 weeks postpartum.

Pregnancy-Related Trigger Finger
Stenosing tenosynovitis at the A1 pulley produces a finger that catches, clicks, or locks. Pregnancy and postpartum trigger finger is more common in patients with diabetes (including gestational diabetes) and in patients with a personal or family history of trigger finger. Multiple fingers may be involved.
General Arthralgias
Generalized joint aches, including in the hands, are common in late pregnancy and early postpartum. Most are non-specific and resolve over weeks. New persistent symmetric joint pain that develops postpartum should be evaluated for postpartum-onset rheumatoid arthritis, particularly when accompanied by morning stiffness greater than 1 hour.
Symptoms and Warning Signs
- Hand numbness or tingling, especially at night, during the second or third trimester
- Thumb-side wrist pain after delivery, particularly when lifting the baby
- A finger that catches, clicks, or locks, particularly the thumb or ring finger
- Pain in the wrist or thumb that worsens with breastfeeding or bottle holding
- Tenderness on direct pressure over the median nerve at the wrist or over the first dorsal compartment
- Pain reproduced by Finkelstein or Eichhoff testing of the thumb
- Symptoms that interfere with sleep or with caring for the baby
- New finger numbness that persists after delivery, particularly with weakness
How the Diagnosis Is Made
Diagnosis is clinical. The standard provocative tests for carpal tunnel and De Quervain's are unchanged in pregnancy. Imaging is selectively used.
- Tinel's sign at the wrist: tapping over the median nerve reproduces tingling in the median distribution.
- Phalen's maneuver: sustained wrist flexion reproduces median symptoms.
- Finkelstein test: the patient makes a fist over the thumb and ulnarly deviates the wrist. Sharp pain at the radial styloid is positive for De Quervain's.
- Eichhoff test: a similar maneuver with the examiner deviating the wrist. Sometimes considered more sensitive than Finkelstein.
- Trigger finger test: palpation of the A1 pulley with the patient flexing and extending the affected finger reveals tenderness, a palpable nodule, and reproduction of the catch.
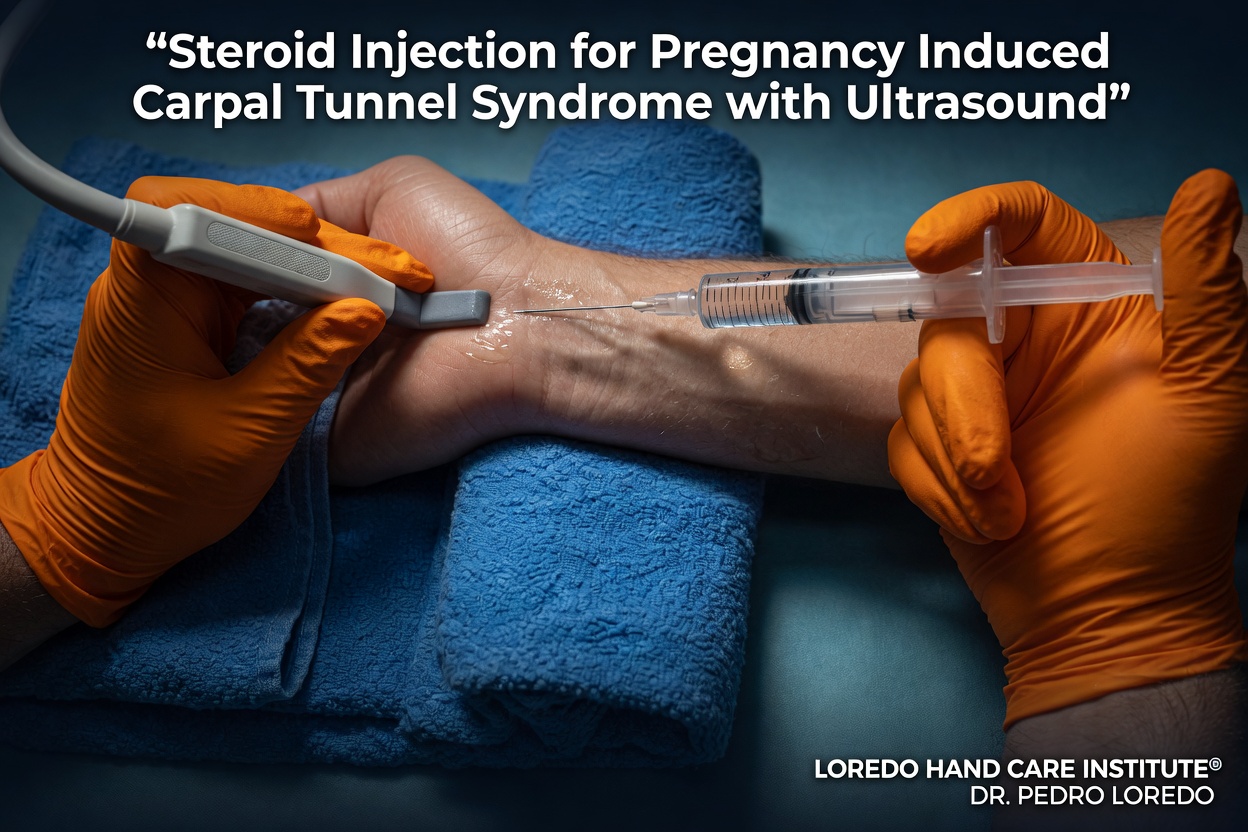
- Ultrasound is the imaging of choice for pregnant patients because it avoids ionizing radiation. It can confirm median nerve enlargement at the carpal tunnel and tendon thickening in the first dorsal compartment.
- Electrodiagnostic studies (EMG and nerve conduction) are appropriate when the diagnosis is uncertain or surgery is being contemplated. They are safe in pregnancy.
Pregnancy-Safe Conservative Treatment
- Wrist night splinting in a neutral position is the most effective single intervention for pregnancy carpal tunnel syndrome. Most patients see substantial improvement within 1 to 2 weeks.
- Thumb spica splinting for postpartum De Quervain's. Off-the-shelf splints are widely available; custom splints from a hand therapist provide the best fit.
- Activity modification: alternate breastfeeding positions, reposition the baby with two hands rather than scooping with the thumb, use a sling or cushion for support, change diapers on a flat surface to avoid prolonged thumb extension.
- Ergonomic infant care: pick up the baby with both hands under the body rather than under the arms with extended thumbs, alternate which hand carries, take micro-breaks every 30 to 60 minutes during long feeding sessions.
- Hand therapy with a certified hand therapist for nerve and tendon gliding exercises and ergonomic instruction.
- Ice 15 to 20 minutes several times a day on the affected area.
- Acetaminophen for short-term symptom relief, in coordination with the OB.
- Topical anti-inflammatories such as topical diclofenac for postpartum patients (avoid in pregnancy).
- Postpartum corticosteroid injection for moderate-to-severe De Quervain's or carpal tunnel symptoms that do not respond to splinting. Single injection often produces 6 to 12 months of relief and may avoid surgery entirely.
When Surgery Is Considered
Surgery is uncommon during pregnancy and is typically deferred until after delivery when possible. Postpartum surgery is appropriate when conservative care has failed for severe symptoms or when symptoms persist beyond 6 to 12 months of structured non-surgical management.
Endoscopic Carpal Tunnel Release
Outpatient minimally invasive procedure through a micro incision at the wrist. Local anesthesia with light sedation. Same-day discharge with a soft dressing and no skin sutures. Most postpartum patients return to baby care within 1 to 2 weeks. See the dedicated Endoscopic Carpal Tunnel Release page for full details.
De Quervain's Release
Outpatient release of the first dorsal compartment through a small incision at the radial wrist. Local anesthesia. Most patients resume light infant care within days and full infant care within 2 to 4 weeks. See the dedicated De Quervain's Tendonitis page for full details.
Trigger Finger Release
Outpatient release of the A1 pulley through a small palmar incision. Same-day return to most light activity. See the dedicated Trigger Finger page for full details.
Recovery Timeline
- Pregnancy carpal tunnel: conservative measures often produce substantial improvement within 1 to 2 weeks. Most cases resolve fully within 4 to 12 weeks of delivery.
- Postpartum De Quervain's: splinting and activity modification produce relief within 2 to 4 weeks for most patients. Single corticosteroid injection produces relief in 70 to 80 percent of cases. Surgery, when needed, has a 90 percent or higher success rate.
- Postpartum trigger finger: often responds to single corticosteroid injection. Surgical release is curative when injection fails.
- Surgery for postpartum carpal tunnel: return to typing and most desk activity within 2 to 7 days. Full infant care within 2 to 4 weeks.
- Surgery for postpartum De Quervain's: return to light infant care within 1 week, full activity within 4 to 6 weeks.
Returning to Baby Care
- Splinting alone: immediate, with the splint on during baby care
- After cortisone injection: immediate, with mild residual splint use as needed
- After endoscopic carpal tunnel release: light baby care within 1 to 2 weeks, full care including bathing within 2 to 4 weeks
- After De Quervain's release: light care within 1 week, full care within 4 weeks
- After trigger finger release: light care within 3 to 5 days, full care within 2 weeks
Frequently Asked Questions
Is hand pain in pregnancy normal?
Hand pain during the second and third trimesters is common and usually not dangerous. Pregnancy-related fluid retention and hormonal changes increase pressure in the carpal tunnel, producing the same numbness, tingling, and night symptoms that classic carpal tunnel syndrome causes. Up to half of pregnant women experience some hand symptoms in the third trimester. Most cases resolve within a few weeks to months after delivery as fluid retention decreases. Severe symptoms, persistent weakness, or symptoms that prevent sleep should be evaluated.
Why do new mothers get thumb pain?
De Quervain's tenosynovitis (sometimes called mommy thumb) is the classic postpartum hand condition. The first dorsal compartment tendons that move the thumb become inflamed from the repetitive lifting that infant care requires: scooping a baby out of a bassinet, supporting the head with the thumb extended, breastfeeding positions, and bottle holding. Postpartum hormonal changes also increase tendon swelling. Symptoms typically begin 4 to 6 weeks after delivery and respond well to splinting, activity modification, and corticosteroid injection.
What is safe to take while I am pregnant or breastfeeding?
Acetaminophen is generally safe in pregnancy and breastfeeding for short-term symptom relief, in coordination with your obstetrician. Most NSAIDs (ibuprofen, naproxen) are avoided in pregnancy, particularly the third trimester, but are usually acceptable while breastfeeding. Topical anti-inflammatory medications cross less placentally and are sometimes preferred. Wrist splints, ice, hand therapy, and ergonomic modifications are pregnancy-safe at any stage and are first-line for most pregnancy hand pain. Always coordinate medication choices with your OB and pediatrician.
Can I have surgery during pregnancy?
Most hand surgery is deferred until after delivery when possible because pregnancy-related hand symptoms often resolve postpartum without intervention. Surgery is reserved for severe symptoms, progressive nerve damage, or threatened tissue loss. When surgery is necessary during pregnancy, the second trimester is the safest window, regional or local anesthesia is preferred over general, and the OB is involved in planning. Most pregnancy carpal tunnel and De Quervain's cases improve enough postpartum that surgery is never needed.
How does Dr. Loredo coordinate with my OB?
For pregnant patients, our office contacts the OB before any procedure or medication change to confirm the plan and obtain any needed clearance. We document fetal age and trimester, choose pregnancy-safe imaging (ultrasound rather than X-ray when possible), and select medications and anesthetic plans appropriate to the gestational age. For postpartum patients, particularly those breastfeeding, we coordinate with the pediatrician on medication choices and timing of injections relative to feedings.
When to Call the Doctor
Call our office for evaluation if you experience:
- Hand numbness or tingling that wakes you at night during pregnancy
- Thumb-side wrist pain that worsens with infant lifting
- A finger that catches, clicks, or locks
- Pain that interferes with caring for your baby
- Symptoms that have not resolved within 8 to 12 weeks of delivery
- Worsening hand symptoms despite splinting and activity modification
- New numbness or weakness that is constant (not just episodic)
Call promptly for any of the following, which suggest a different diagnosis:
- Constant hand numbness with visible thumb muscle thinning (severe carpal tunnel)
- New symmetric joint pain with morning stiffness more than 1 hour (postpartum-onset RA)
- Sudden severe pain or color change in the fingers (suspect Raynaud's or vascular issue)
- Fever, rash, or systemic illness with the hand symptoms
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Carpal Tunnel Syndrome: the most common cause of pregnancy hand numbness. Full discussion of diagnosis, treatment options, and the endoscopic release procedure.
- De Quervain's Tendonitis: the dedicated page for first dorsal compartment tenosynovitis, including the postpartum mommy thumb pattern.
- Trigger Finger: stenosing tenosynovitis at the A1 pulley. More common in pregnancy and postpartum, particularly in patients with diabetes.
- Hand and Wrist Arthritis: postpartum-onset rheumatoid arthritis is a recognized presentation. Differentiate from non-specific arthralgias by symmetric joint involvement and prolonged morning stiffness.
- Raynaud's Disease: sudden cold-induced finger color changes occasionally appear or worsen during pregnancy or postpartum.
From the Blog
- Early Signs of Carpal Tunnel: the third-trimester symptoms most pregnant patients face.
- Night Splints for Carpal Tunnel: the first-line treatment in pregnancy.
- When a Cortisone Injection Is the Right Choice: timing considerations during and after pregnancy.
Watch: Pregnancy and postpartum hand pain education
Short videos from Dr. Loredo's Instagram and Facebook channels.