Raynaud's disease, also called Raynaud's phenomenon, is episodic vasospasm of the small arteries that supply the fingers (and sometimes toes, ears, and nose). Cold exposure or emotional stress triggers a brief but intense constriction of these arteries, producing the classic triphasic color change of white (vasospasm), blue (cyanosis), and red (reperfusion). The condition is divided into primary Raynaud's (idiopathic, more common, generally benign) and secondary Raynaud's (associated with systemic disease such as scleroderma, lupus, or rheumatoid arthritis, or with chronic vibration exposure). Treatment ranges from aggressive cold avoidance and oral calcium channel blockers to digital sympathectomy and arteriolysis in refractory cases with tissue at risk.
The Vascular Anatomy of the Finger
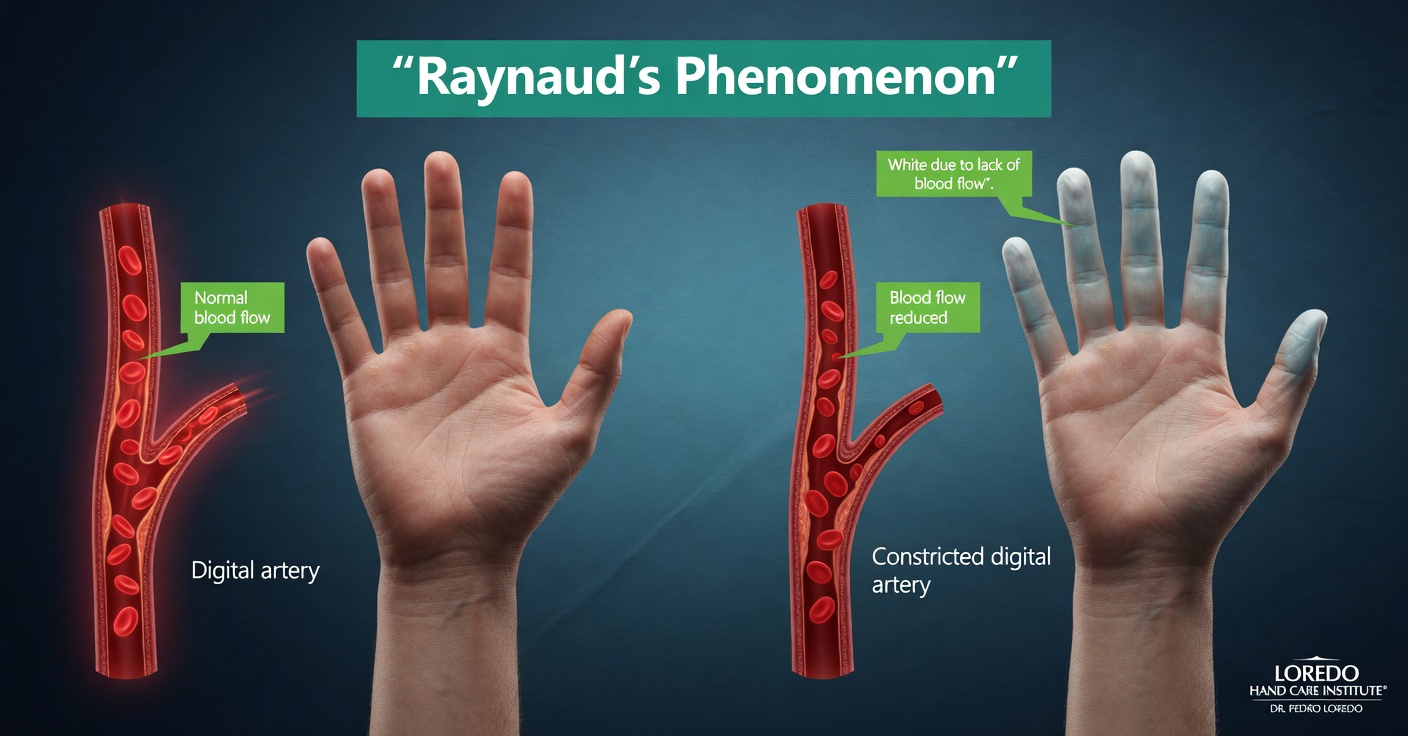
Each finger receives blood through two digital arteries that run along the radial and ulnar sides. These arteries arise from the superficial palmar arch in the palm and divide into smaller arterioles that supply the skin, nail bed, and pulp tissue at the fingertip. Sympathetic nerve fibers travel along these arteries and control their diameter through smooth muscle in the arterial wall.
In Raynaud's, the smooth muscle in the digital arteries becomes hyper-responsive to cold and to sympathetic outflow. Modest cold exposure that would produce a small amount of normal vasoconstriction in most people instead produces a near-complete shutdown of arterial flow. The downstream tissue becomes ischemic for the duration of the attack. Most attacks resolve within 15 to 30 minutes, but severe or prolonged episodes can produce small areas of skin ulceration at the fingertips, and in advanced secondary Raynaud's, frank gangrene with tissue loss.
The thumb is anatomically protected from Raynaud's because its vascular supply differs slightly from the other digits. Thumb involvement should always raise suspicion for secondary Raynaud's and an underlying systemic disease.
Clinical coding: ICD-10 I73.00 (Raynaud's syndrome without gangrene), I73.01 (with gangrene). SNOMED CT 195295006.
Primary Versus Secondary Raynaud's
- Primary Raynaud's typically begins between ages 15 and 30, affects women 4 times more often than men, and is symmetric (both hands equally). There is no underlying systemic disease. Primary Raynaud's is generally benign and rarely produces ulceration or tissue loss. Most patients have a family history.
- Secondary Raynaud's begins later in life, may be asymmetric, can involve the thumb, and is associated with an underlying systemic illness. The most common associated diseases are scleroderma, systemic lupus erythematosus, mixed connective tissue disease, Sjögren's syndrome, and rheumatoid arthritis. Vibration tool use, certain medications, and obstructive vascular disease (such as thoracic outlet syndrome with subclavian artery aneurysm) are also recognized causes. Secondary Raynaud's is more likely to produce digital ulcers and tissue loss and warrants rheumatology evaluation.
Causes and Risk Factors
- Cold exposure in any setting (refrigerator, air-conditioned room, fall or winter weather)
- Emotional stress through sympathetic outflow
- Smoking and tobacco use, which directly impair small vessel vasodilation
- Vibration tool use (jackhammers, grinders, chainsaws), causing acquired secondary Raynaud's
- Medications including beta-blockers, ergot derivatives, ADHD stimulants, certain migraine treatments, and some chemotherapy drugs
- Caffeine can lower the threshold for attacks in sensitive patients
- Connective tissue disease, particularly scleroderma (where Raynaud's is often the first symptom and may precede the systemic diagnosis by years)
- Family history of Raynaud's
- Female sex (4 times more common than men in primary disease)
Symptoms and Warning Signs
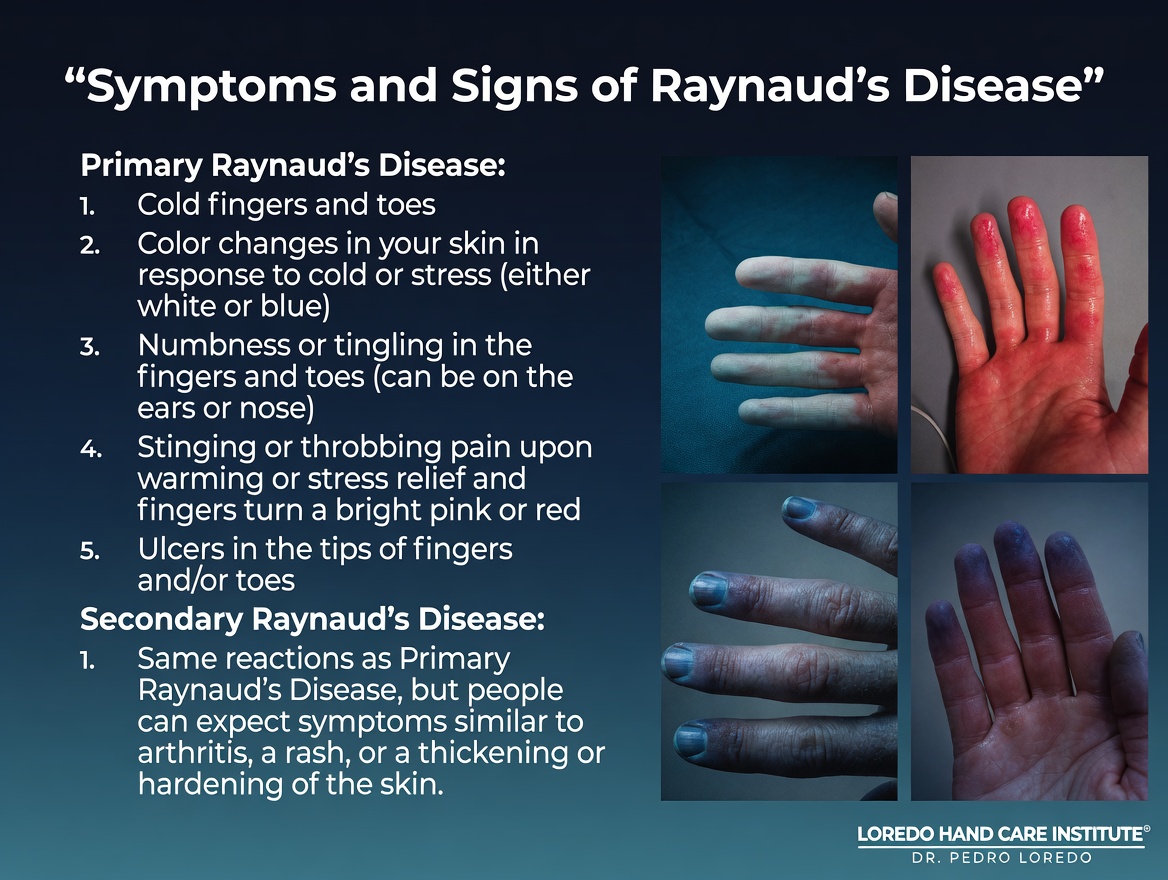
- Episodic finger color change triggered by cold or stress, classically passing through white, blue, and red phases
- Cold or numb fingers during the white phase, sometimes with sharp pain
- Tingling or burning during the red reperfusion phase
- Symptoms typically affecting multiple fingers symmetrically
- Thumb sparing in primary disease (thumb involvement suggests secondary)
- Digital ulcers, particularly at the fingertips, in severe disease
- Pitted scars or healed ulcerations from prior attacks
- Skin tightening or thickening of the fingers (suggests scleroderma)
- In advanced secondary Raynaud's, frank gangrene at the fingertip
How the Diagnosis Is Made
Raynaud's is a clinical diagnosis based on the history of episodic triphasic color change. Most patients can describe or photograph an attack, which is the most useful single piece of diagnostic information.
- History of triphasic color change: the pale white phase is most diagnostic. Two of the three colors are required for diagnosis; all three are not necessary.
- Cold provocation test: immersing the hands in cool water can reproduce an attack in the office, though most patients prefer to bring photos taken at home.
- Nailfold capillaroscopy: microscopic examination of the capillaries at the cuticle. Abnormal patterns (dilated capillaries, drop-out areas, hemorrhages) suggest secondary Raynaud's and connective tissue disease and prompt rheumatology referral.
- Laboratory studies when secondary Raynaud's is suspected: ANA panel, ESR, CRP, complement levels, anti-Scl-70, anti-centromere antibodies, anti-RNP. A positive workup is the single strongest predictor of progression to a defined connective tissue disease.
- Imaging in selected cases: ultrasound or angiography to exclude proximal large-vessel disease, particularly when symptoms are unilateral or asymmetric.
Non-Surgical Treatment Options
The great majority of Raynaud's patients are well controlled with conservative measures and do not need surgery.
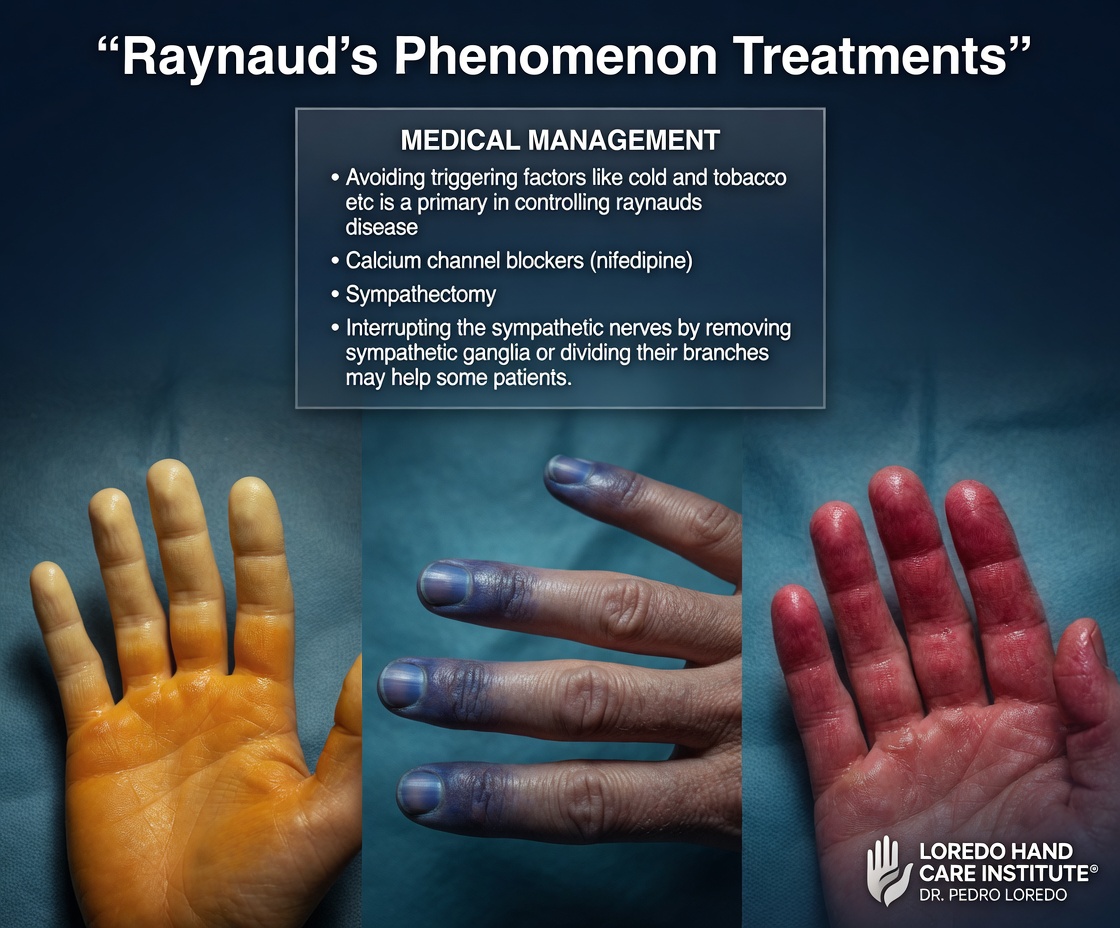
- Aggressive cold avoidance: the foundation of all Raynaud's care. Layer gloves under mittens, use chemical hand warmers, keep the trunk warm to prevent reflex hand vasoconstriction, avoid handling cold drinks or refrigerator items without insulated gloves.
- Smoking cessation is non-negotiable. Tobacco use directly worsens vasoconstriction and is the most reversible risk factor.
- Stress management and biofeedback when emotional triggers are prominent.
- Avoidance of triggering medications when possible. Coordinate any change with the prescribing physician.
- Calcium channel blockers are first-line oral therapy. Nifedipine and amlodipine are most commonly used and reduce attack frequency and severity in most patients. Side effects include headache, ankle edema, and flushing.
- Topical nitrates (nitroglycerin ointment 0.4 percent or 2 percent) applied to the affected fingers during attacks or as a daily maintenance therapy.
- Phosphodiesterase-5 inhibitors (sildenafil, tadalafil) for refractory disease, particularly in patients with scleroderma-associated Raynaud's.
- Prostacyclin analogs (intravenous iloprost or treprostinil) are reserved for severe disease with critical ischemia and are typically managed by rheumatology or vascular medicine.
- Botulinum toxin injection at the base of the affected fingers can reduce sympathetic vasoconstriction for 3 to 6 months and is a useful adjunct or bridge to surgical sympathectomy.
Surgical Options
Surgery is reserved for severe refractory secondary Raynaud's with critical digital ischemia, persistent ulcers, or threatened tissue loss. Most patients never need surgery.
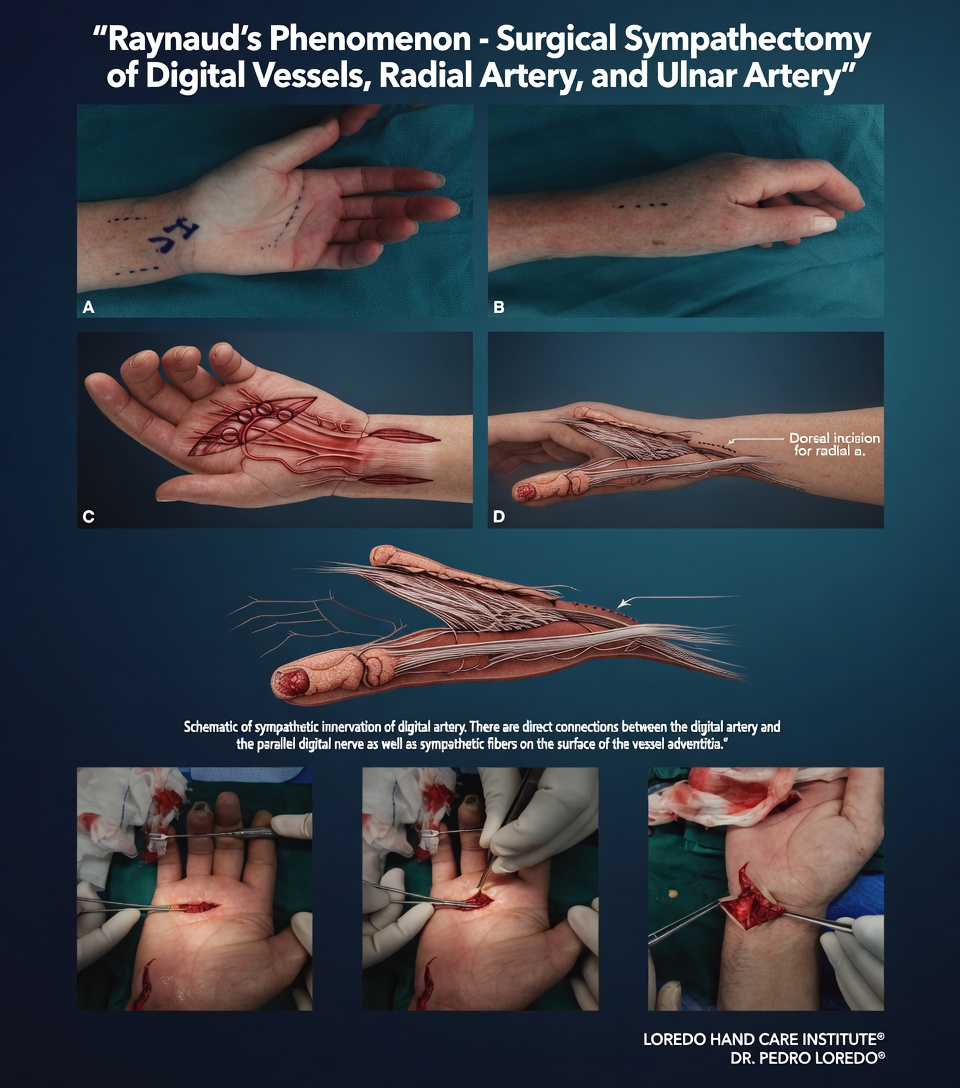
Digital Sympathectomy and Arteriolysis
- Microsurgical procedure performed under loupe or microscope magnification
- Small incision at the base of each affected finger
- The digital arteries are exposed and the sympathetic nerve fibers traveling along the artery wall are stripped (adventitial stripping)
- Removing the sympathetic input eliminates the signal that drives vasospasm at that finger
- Procedure takes 1 to 2 hours per finger under regional or general anesthesia
- Soft dressing and gentle splint for the first week
- Outcomes show 60 to 80 percent improvement in pain and ulcer healing in carefully selected patients
Botulinum Toxin Injection
Often performed in the same setting as a planned sympathectomy or as a stand-alone office procedure. Botox injection at the base of the affected fingers blocks sympathetic neurotransmission for 3 to 6 months and is a useful trial before committing to permanent sympathectomy.
Other Procedures
Debridement of digital ulcers, revascularization of compromised tissue, and revision amputation when tissue loss is irreversible are occasionally needed in advanced disease.
Recovery Timeline
- Conservative management: attack frequency typically decreases within 2 to 4 weeks of starting calcium channel blockers and aggressive cold avoidance.
- Botulinum toxin injection: effect onset within 1 to 2 weeks, peak at 3 to 4 weeks, duration 3 to 6 months.
- Digital sympathectomy: dressing and splint for 1 week, gentle motion at week 2, full activity at 4 to 6 weeks.
- Ulcer healing: small fingertip ulcers heal over 4 to 8 weeks with appropriate wound care; larger or deeper ulcers may take 3 to 6 months.
Returning to Work and Daily Activity
- Office or desk work: within days for medication starts; 1 to 2 weeks after sympathectomy
- Light manual labor: 2 to 4 weeks after sympathectomy
- Outdoor work or cold-exposed work: requires aggressive cold protection year-round; 4 to 6 weeks after sympathectomy
- Vibration tool work: ideally avoided permanently in patients with vibration-induced secondary Raynaud's
- Driving: 1 to 2 weeks after sympathectomy
Frequently Asked Questions
What is the difference between primary and secondary Raynaud's?
Primary Raynaud's (also called Raynaud's disease) occurs without an underlying systemic illness. It is far more common, typically begins in younger women (15 to 30), is symmetric, and rarely causes tissue damage. Secondary Raynaud's occurs in the setting of a systemic disease (most commonly scleroderma, lupus, rheumatoid arthritis, or Sjögren's syndrome) or after vibration exposure. Secondary Raynaud's tends to be more severe, more asymmetric, more likely to cause digital ulcers, and may signal undiagnosed connective tissue disease that warrants rheumatology evaluation.
Why do my fingers turn three different colors?
The classic Raynaud's attack has three phases. First, white: small arteries in the fingers spasm and shut down blood flow, leaving the affected fingers pale. Second, blue: deoxygenated blood pools in the static capillaries, turning the fingers cyanotic. Third, red: the spasm releases and reperfusion brings a flush of bright red blood back. Not every patient gets all three phases, and the white phase is the most diagnostic. Many patients describe pain or numbness during the white phase and tingling or burning during the red phase.
What can trigger an attack?
Cold exposure is the most common trigger. Even modest cold (a refrigerator, an air-conditioned room, walking outside in fall weather) can provoke an attack in sensitive patients. Other triggers include emotional stress, smoking, certain medications (beta-blockers, ergot derivatives, ADHD stimulants, some migraine treatments), and chronic vibration tool use. Caffeine can also lower the threshold for attacks in some patients.
When do I need to see a hand surgeon?
Most Raynaud's patients are managed by a primary care physician or rheumatologist with conservative measures and oral medications. A hand surgeon becomes involved when severe Raynaud's produces digital ulcers that will not heal, when fingertip ischemia threatens tissue loss, when secondary Raynaud's progresses to gangrene, or when conservative and oral therapy have failed and surgical sympathectomy or arteriolysis is being considered. Coordination with rheumatology and vascular medicine is the rule rather than the exception in advanced cases.
What does sympathectomy involve?
Digital sympathectomy and arteriolysis is a microsurgical procedure that strips the sympathetic nerve fibers from the small arteries at the base of the affected finger. Removing these fibers eliminates the signal that causes vasospasm and improves blood flow to the fingertip. The procedure is performed under microscope, takes 1 to 2 hours per finger, and is reserved for severe refractory disease with imminent or actual tissue loss. Many patients also receive Botox injections in the same area for short-term relief while recovery progresses.
When to Call the Doctor
Call our office for evaluation if you experience:
- Triphasic finger color change with cold exposure or stress, particularly if it is new or worsening
- Asymmetric symptoms or thumb involvement (suspect secondary Raynaud's)
- Digital ulceration or pitted scars at the fingertips
- Severe attacks that interfere with daily activity
- Failure of cold avoidance and over-the-counter measures
- Skin tightening or thickening on the fingers (suspect scleroderma)
- Joint pain, dry eyes, dry mouth, or other systemic symptoms with Raynaud's
Call promptly or seek emergency care for:
- A finger that remains pale and painful for more than 30 minutes despite warming
- Black or dark blue discoloration that does not resolve (suspect gangrene)
- Open ulcer with thick, yellow, or foul-smelling drainage
- Fever, chills, or systemic illness in the setting of a digital ulcer
Critical digital ischemia or gangrene is an emergency. Call 911 or go to the nearest emergency department immediately.
Related Conditions
- Hand and Wrist Arthritis: rheumatoid arthritis is one of the connective tissue diseases associated with secondary Raynaud's. Joint and skin findings are commonly evaluated together.
- Carpal Tunnel Syndrome: can coexist with Raynaud's, particularly in patients with diabetes or scleroderma. Cold-induced numbness from Raynaud's is sometimes confused with median nerve compression.
- Cubital Tunnel Syndrome: ulnar nerve compression that can produce ring and small finger numbness, occasionally confused with Raynaud's in atypical presentations.
- Guyon's Canal Syndrome: handlebar palsy in cyclists who also experience cold-induced symptoms. Differentiated by the absence of triphasic color change in pure nerve compression.
- Hand and Finger Fractures: rare cases of post-traumatic vascular insufficiency can mimic Raynaud's at the affected finger.
From the Blog
- Ergonomic Tips for Hand Pain: glove use and cold-exposure strategies.
Watch: Raynaud's phenomenon education
Short videos from Dr. Loredo's YouTube and Facebook channels.