Thumb CMC reconstruction (basilar joint arthroplasty) is the workhorse surgical treatment for advanced thumb carpometacarpal arthritis. Dr. Loredo offers several technique options: trapeziectomy alone, trapeziectomy with ligament reconstruction tendon interposition (LRTI) using the FCR tendon, suture suspension arthroplasty (Mini-TightRope, FlexBand, and similar devices), and selected pyrocarbon implant arthroplasty. All approaches share a common goal: remove the arthritic trapezium and stabilize the thumb metacarpal in its anatomic position. The procedure takes 60 to 90 minutes under regional or general anesthesia. A thumb spica splint is worn for 4 to 6 weeks, followed by 6 to 12 weeks of structured hand therapy. Long-term outcomes show 90 percent or higher patient satisfaction, with most patients describing dramatic relief of the pain that defined their daily life before surgery.
What Is CMC Reconstruction?
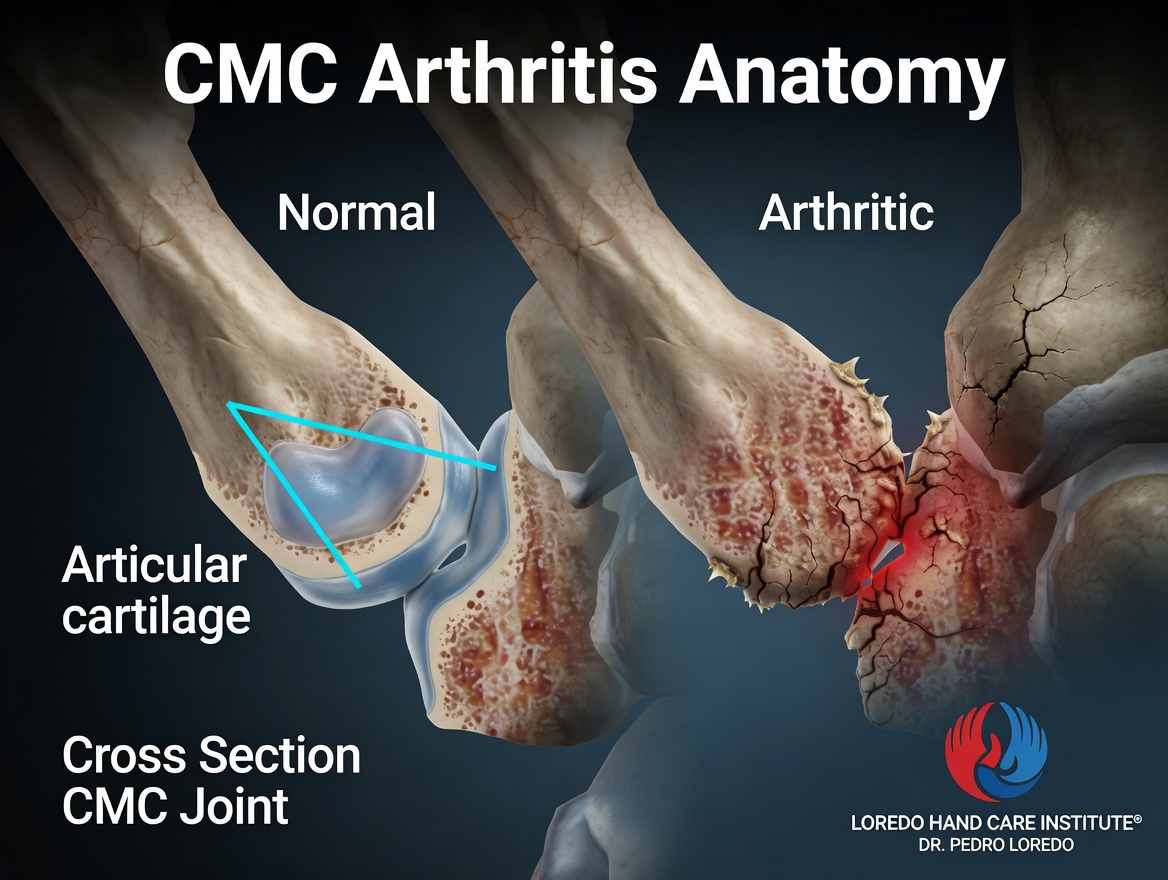
The thumb carpometacarpal (CMC) joint, also called the basilar joint, sits at the base of the thumb where the thumb metacarpal articulates with the trapezium carpal bone. The joint is a saddle-shaped articulation that allows the thumb to oppose the fingers, the motion that defines human hand function. Decades of pinching, gripping, and load wear the cartilage of this joint, producing thumb base arthritis. Patients describe deep aching pain at the thumb base that worsens with opening jars, turning a key, pinching small objects, and gripping tools.
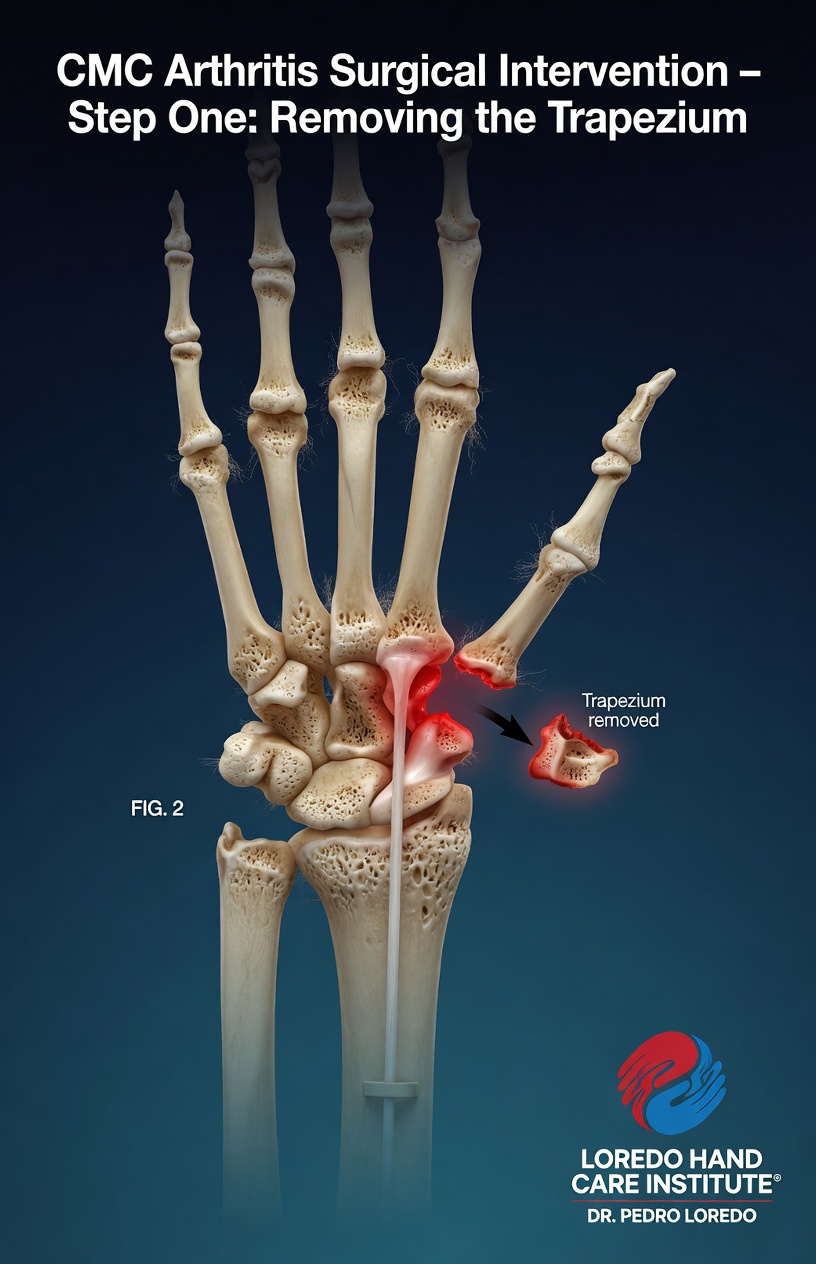
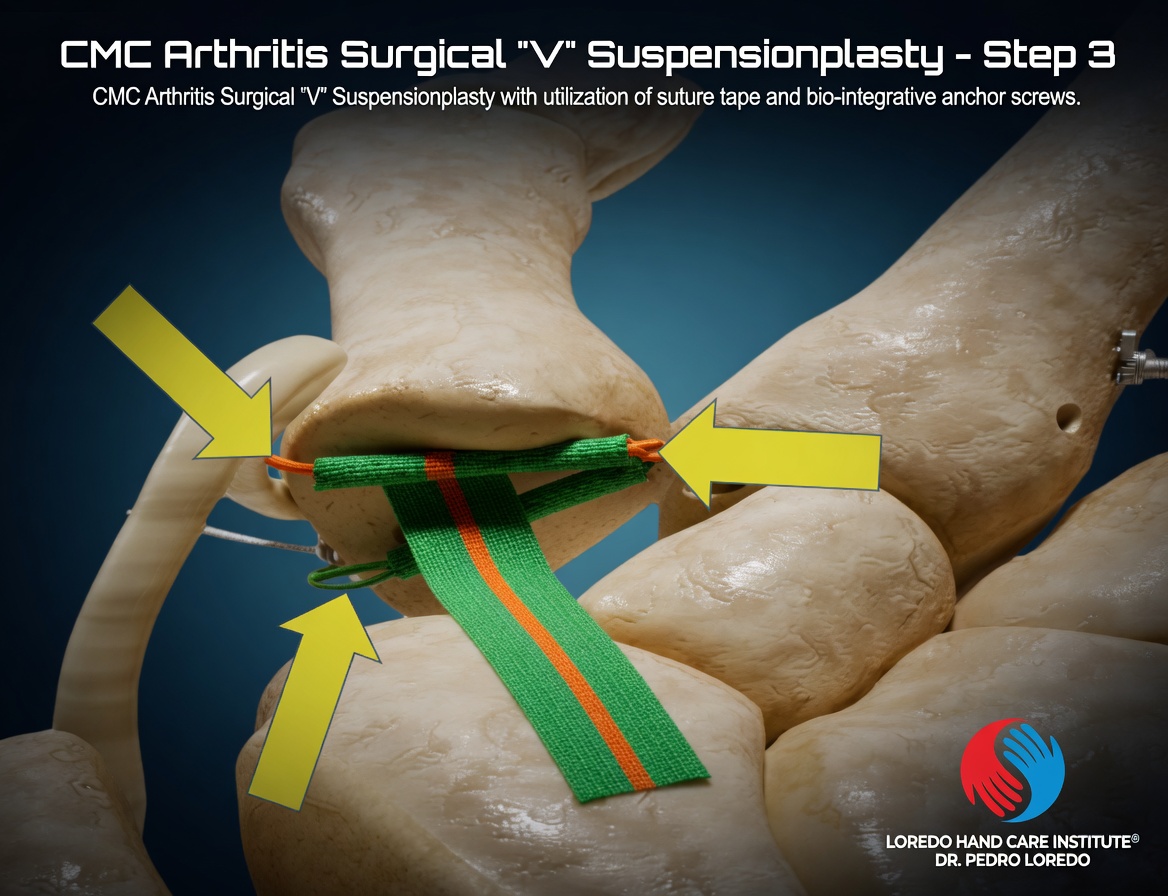
CMC reconstruction surgically addresses the arthritic joint. The trapezium is removed (trapeziectomy), eliminating the bone-on-bone contact that produces pain. The thumb metacarpal is then stabilized in the resulting space. Dr. Loredo's primary surgical approach is a modern V-configuration Suture Suspensionplasty using suture tape and bio-integrative anchor screws. This technique stabilizes the thumb metacarpal in proper anatomic position without harvesting the FCR tendon and uses anchor screws that gradually integrate with the patient's own bone. The traditional alternative, LRTI (Ligament Reconstruction Tendon Interposition), uses a folded strip of the FCR tendon and remains an option when patient anatomy or specific clinical factors favor it. For full background on the underlying condition, see Thumb Basilar Joint Arthritis.
Who Is a Candidate?
- Thumb base pain confirmed by examination, with positive grind test and tenderness over the CMC joint
- X-ray evidence of advanced thumb CMC arthritis (Eaton stage III or IV)
- Failure of conservative care including activity modification, splinting, and at least one corticosteroid injection
- Pain that limits work, daily activities, or sleep
- Loss of pinch strength sufficient to interfere with daily function
- Patient preference for definitive surgical correction over ongoing conservative management
How the Procedure Is Performed
Dr. Loredo's primary surgical approach is a four-step V-configuration Suture Suspensionplasty:
- Positioning and anesthesia. The patient lies supine with the affected arm extended on a hand table. Regional anesthesia or general anesthesia is used.
- Incision. A curved or longitudinal incision is made over the dorsoradial thumb base. The radial sensory nerve branches and the radial artery are carefully identified and protected.
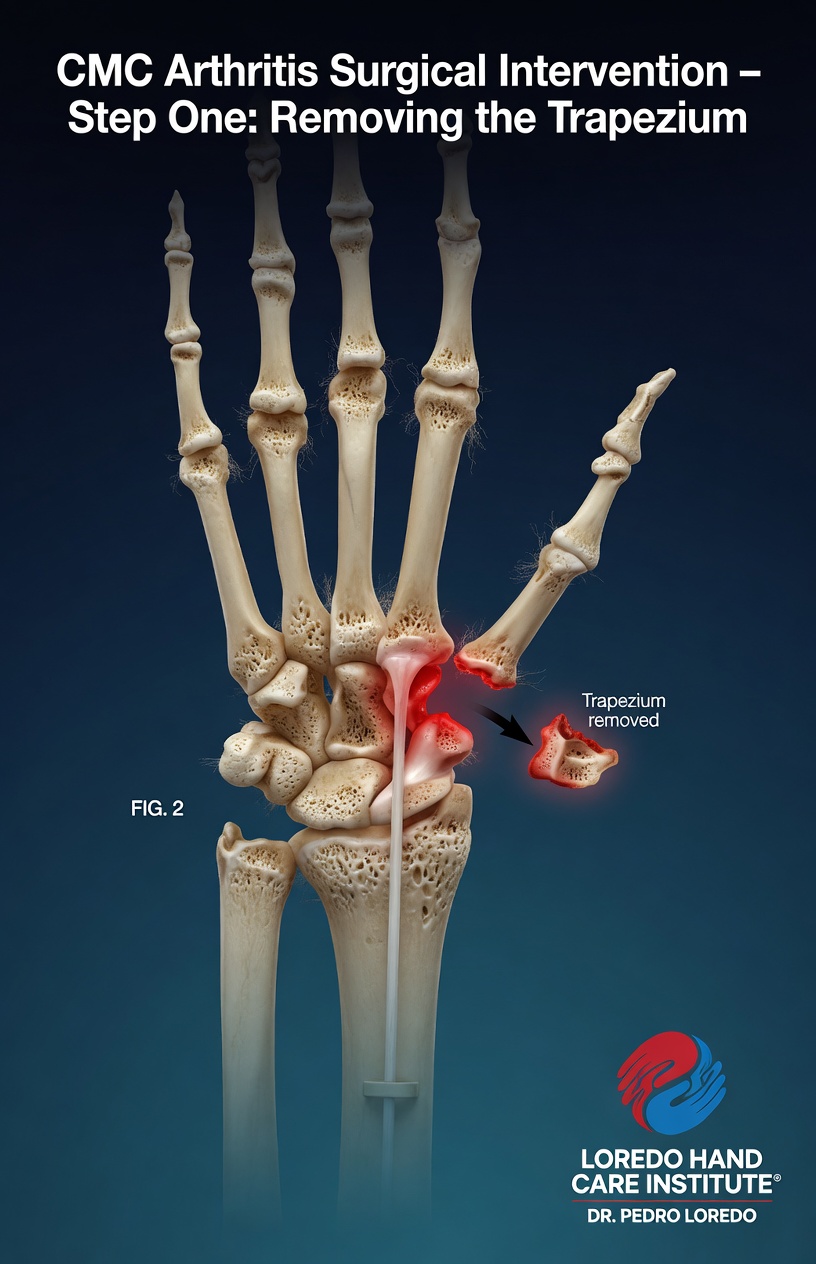
- Trapeziectomy. The trapezium is exposed and removed completely, eliminating the arthritic joint surfaces.
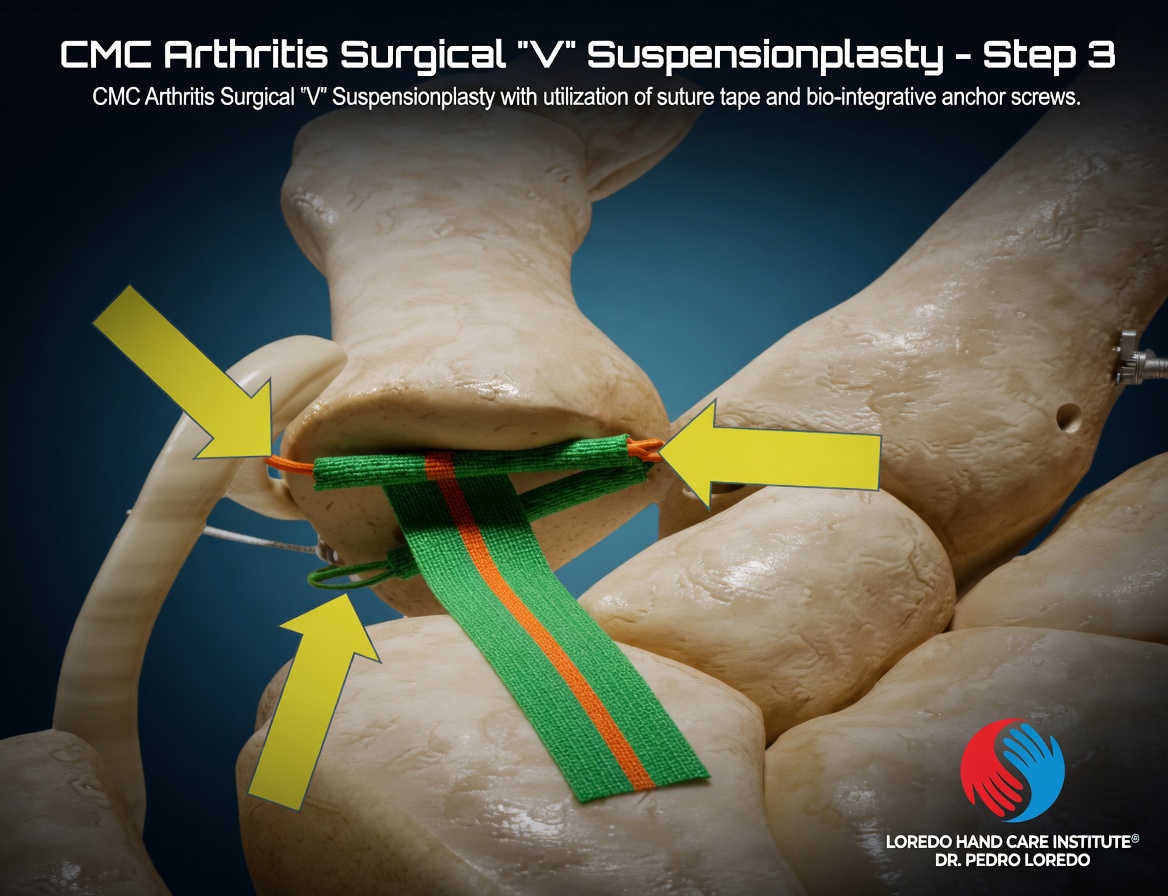
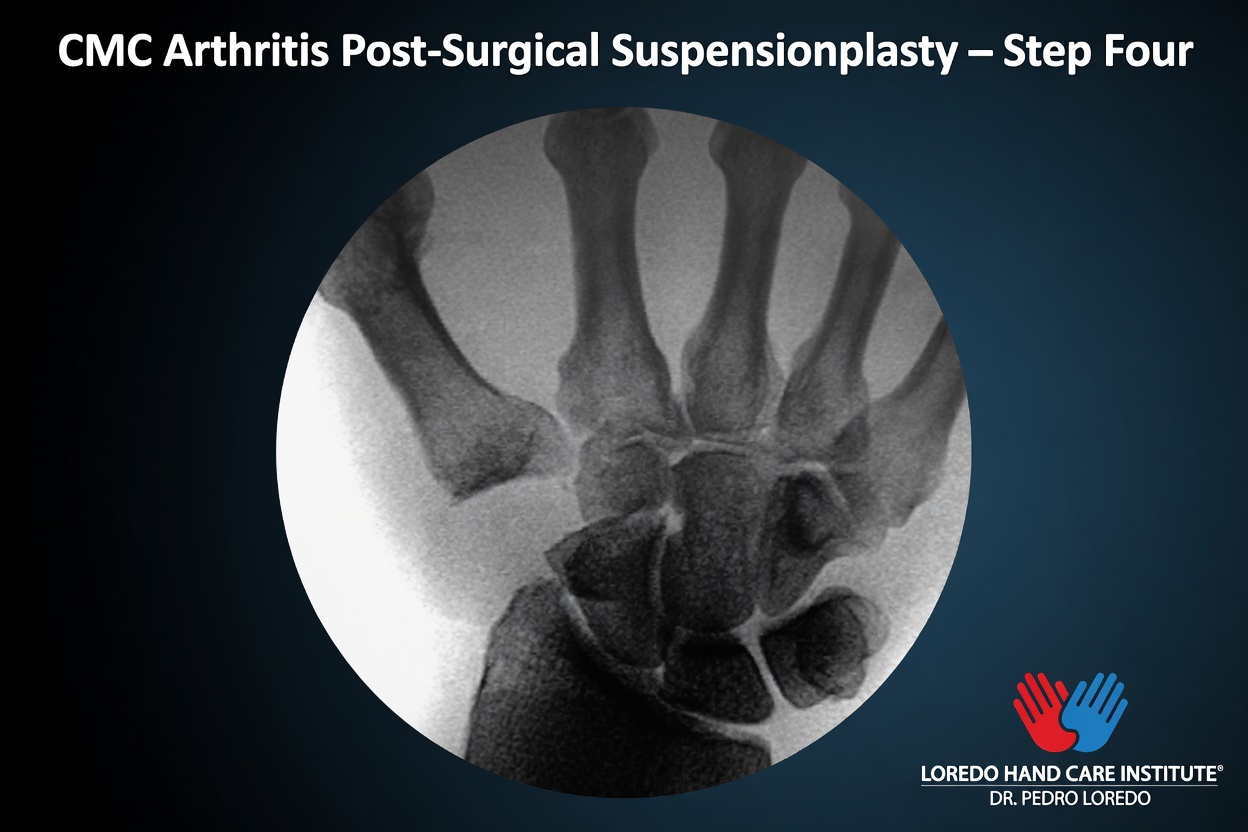
- Suture Suspensionplasty (Dr. Loredo's primary technique). Bio-integrative anchor screws are placed in adjacent stable bone. High-strength suture tape is woven in a V-configuration between the anchors to suspend the thumb metacarpal in proper anatomic position. The bio-integrative anchors gradually convert to bone over time, leaving no permanent foreign material long term. No FCR tendon is harvested.
- Alternative stabilization techniques available when clinically indicated:
- LRTI: a strip of the FCR tendon is harvested from the volar wrist, passed through a tunnel in the thumb metacarpal, used to reconstruct the volar beak ligament, and folded into the trapeziectomy space as an interposition.
- Pyrocarbon implant: a custom synthetic implant is placed in the trapeziectomy space.
- Closure. Capsule and skin are closed in layers. A short arm thumb spica splint is applied.
The Four Surgical Steps Visualized

Anesthesia Options
- Regional axillary or supraclavicular block: the entire arm is numbed for 12 to 18 hours. Most common option for CMC reconstruction.
- General anesthesia: appropriate for patients with anxiety, certain medical conditions, or patient preference.
- Combined regional plus light sedation: regional block plus light IV sedation for additional comfort during the procedure.
Procedure Duration and Setting
The actual surgical time is 60 to 90 minutes. Total time at the surgery center is 3 to 4 hours including check-in, anesthesia, surgery, and recovery. The procedure is performed at an accredited ambulatory surgery center. Discharge is the same day. A family member or friend drives you home.
Recovery Timeline

- Day 0 to 7: Thumb spica splint or short arm cast. Elevation and ice. Pain managed with prescribed medication transitioning to NSAIDs by end of week 1.
- Week 1: First post-operative visit. Sutures inspected. Splint changed if needed.
- Week 2 to 4: Continued splint or cast. Sutures removed at 2 weeks if not absorbable.
- Week 4 to 6: Splint removed. Begin gentle thumb range of motion under hand therapy guidance. Light pinch and grasp activities introduced.
- Week 6 to 12: Progressive thumb strengthening and functional use. Hand therapy continues. Most patients describe substantial pain relief by week 6 to 8.
- Months 3 to 6: Full strengthening. Most patients return to normal activities including work and sport.
- Year 1: Continued functional improvement. Long-term outcomes are excellent.
Return to Work and Daily Activities
- Office or desk work in a splint: 1 to 2 weeks
- Light manual labor: 6 to 8 weeks
- Heavy manual labor and forceful pinch: 12 to 16 weeks
- Driving: 4 to 6 weeks once out of the splint and able to grip the wheel safely
- Sports involving thumb gripping: 4 to 6 months with progressive return
Why CMC Reconstruction Is the Workhorse Procedure
- Durable pain relief: long-term studies show 90 percent or higher patient satisfaction at 10 to 20 years across reconstruction techniques.
- Restored thumb function: opposition, pinch, and grip return to 80 to 90 percent of normal contralateral.
- Low reoperation rate: revision surgery is uncommon.
- Modern Suture Suspensionplasty advantages: no FCR tendon harvest, bio-integrative anchors that convert to bone over time, and faster return to hand use compared to traditional LRTI.
- Multiple technique options allow Dr. Loredo to tailor the reconstruction to patient anatomy, age, activity level, and personal preference.
Risks and Complications
CMC reconstruction is a major hand surgery with a longer recovery than the smaller endoscopic procedures. Recognized risks include:
- Radial sensory nerve injury: branches run directly through the surgical area. Numbness in a patch of skin on the dorsal thumb is a recognized risk; usually resolves over months.
- Radial artery injury (rare): the radial artery passes near the trapezium and is identified and protected.
- Infection (1 to 2 percent): treated with antibiotics; rarely requires reoperation.
- Loss of fixation or subsidence in suture suspension or implant variants: rare with current techniques.
- FCR tendon weakness after LRTI: a portion of the FCR is harvested. Long-term wrist function is preserved because of the FCU and palmaris longus, but transient wrist tenderness is expected.
- Persistent pain or stiffness: uncommon but possible, particularly in patients with widespread upper extremity arthritis.
- Complex regional pain syndrome (CRPS): rare but recognized after any thumb base surgery.
- Anesthesia-related risks: standard for regional or general anesthesia.
Cost and Insurance
CMC reconstruction (CPT 25447 LRTI; other CPT codes for suspension arthroplasty and implant variants) is covered by virtually all commercial insurance plans, Medicare, and Texas workers' compensation when the diagnosis is appropriately documented. The total cost includes the surgeon fee, the surgery center facility fee, and the anesthesia fee. Out-of-pocket cost depends on your specific plan, deductible, and copay. Our team verifies your benefits before surgery. Call our office at (972) 939-4974 for a benefits check.
Frequently Asked Questions
What is the difference between LRTI and suture suspension arthroplasty?
Both procedures begin with trapezium removal (trapeziectomy). LRTI (ligament reconstruction tendon interposition) uses a strip of the FCR tendon to reconstruct the volar beak ligament and to fill the space left by the removed bone. Suture suspension arthroplasty (Mini-TightRope, FlexBand, and similar devices) uses a suture-button construct between the thumb metacarpal and index metacarpal to hold the thumb position without using a tendon. Both have excellent long-term outcomes. LRTI is the longest-studied option with decades of follow-up. Suture suspension is newer, has shorter recovery in some studies, and avoids using the FCR tendon. The choice depends on patient anatomy, hand surgeon experience, and patient preference.
How long until I can use my hand normally?
Recovery from CMC reconstruction is gradual. The thumb spica splint or cast is worn for 4 to 6 weeks. Hand therapy starts at 4 to 6 weeks and continues for 6 to 12 weeks with progressive thumb range of motion and strengthening. Light pinch and grasp activities resume at 6 to 8 weeks. Full strength returns at 3 to 6 months. Most patients describe substantial improvement in pain by 6 to 8 weeks and continued functional improvement through the first year.
Will I lose strength in my thumb?
Most patients gain strength compared to their pre-operative state because the pain that limited grip and pinch is gone. Compared to a normal thumb without arthritis, the operated thumb may be slightly weaker, with most patients ending up at 80 to 90 percent of normal contralateral strength. The functional outcomes are excellent: opening jars, gripping tools, and using the thumb for daily tasks all return.
How long do the results last?
CMC reconstruction is one of the most durable procedures in hand surgery. Long-term studies of LRTI show 90 percent or higher patient satisfaction at 10 to 20 years. Reoperation for any cause is uncommon. Patients typically describe the results as life-changing because thumb base arthritis is so disabling. Pyrocarbon implant arthroplasty has somewhat shorter follow-up data and higher revision rates in some series; LRTI remains the most studied workhorse procedure.
Do I need to try injections first?
Yes, in most cases. Conservative care includes activity modification, splinting (a custom thumb spica splint is most useful), oral and topical anti-inflammatories, hand therapy, and corticosteroid injection. Most patients have at least one injection trial before surgery. Surgery is appropriate when conservative measures have failed, when pain limits work or daily life, and when imaging shows established arthritis with bone-on-bone changes. The transition from conservative care to surgery is a shared decision.
Related Conditions
- Thumb Basilar Joint Arthritis: the underlying condition this procedure treats.
- Hand and Wrist Arthritis: broader discussion of the various forms of hand arthritis.
- De Quervain's Tendonitis: thumb-side wrist condition that can coexist with CMC arthritis and is sometimes addressed in the same setting.
- Trigger Finger: frequently coexists with CMC arthritis in patients with diabetes or rheumatoid disease.
Related Procedures
- De Quervain's Release: occasionally combined with CMC reconstruction when both conditions are present.
- Open A1 Pulley Release for Trigger Finger: same-session option for coexisting trigger thumb.
- Endoscopic Carpal Tunnel Release: combined surgery is appropriate when both conditions limit hand function.
- All Procedures: the full list of surgical procedures offered at the practice.
From the Blog
- CMC Arthroplasty Recovery: thumb spica weeks 1 to 6, hand therapy, full strength at 3 to 6 months.
- Thumb Arthritis: When Injections Stop Working: the path that leads to surgical reconstruction.
- The Basal Joint of the Thumb: why CMC reconstruction differs from joint replacement.
Watch: Thumb CMC reconstruction education
Short videos from Dr. Loredo's Instagram and Facebook channels.