De Quervain's release is a surgical decompression of the first dorsal compartment at the radial wrist for De Quervain's tenosynovitis. Through a small transverse incision over the radial styloid, Dr. Loredo first identifies and protects the branches of the superficial radial nerve that cross the surgical field, then divides the retinaculum overlying the compartment and releases all sub-sheaths so the APL and EPB tendons can glide freely. The procedure takes 15 to 30 minutes under local anesthesia only, in either the office surgical suite or an ambulatory surgery center. Most patients use the hand within 1 to 2 days, return to most activity within 2 to 4 weeks, and rarely need formal hand therapy.
What Is De Quervain's Release?
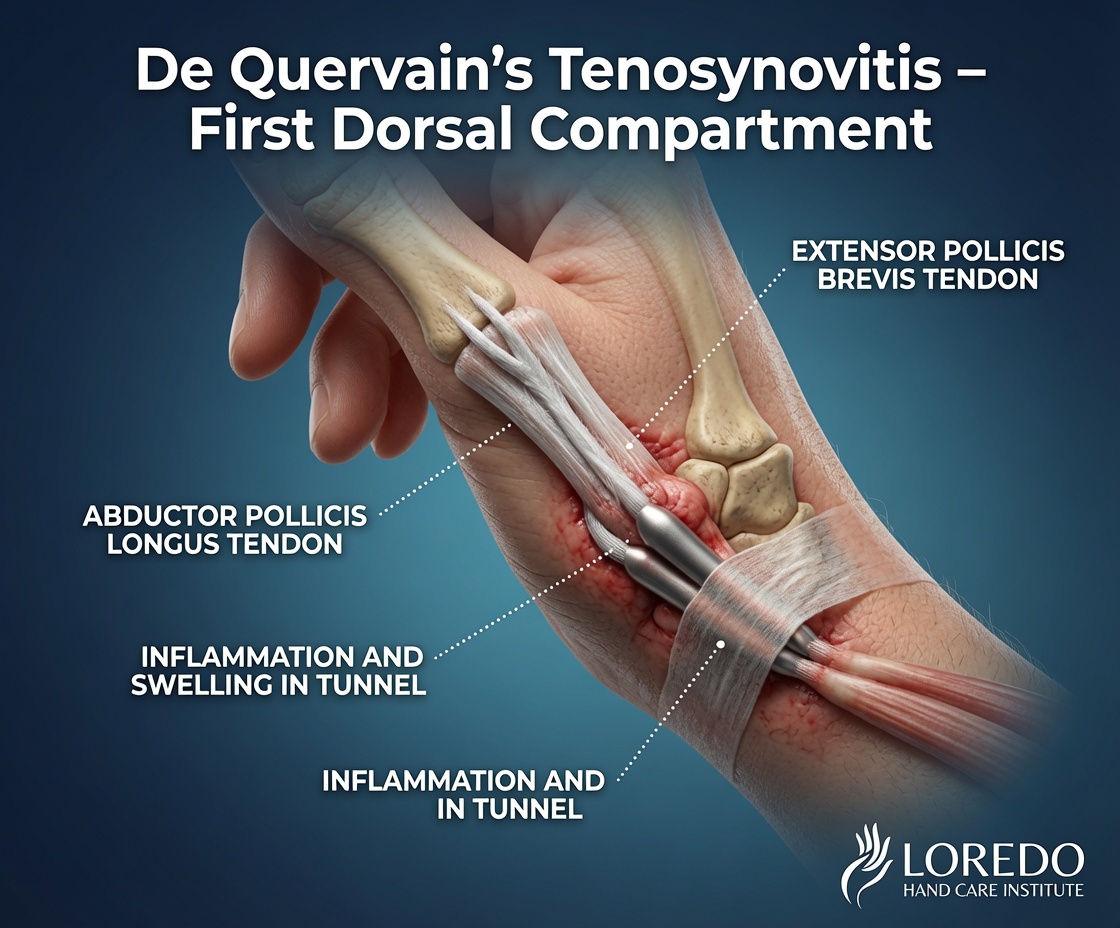
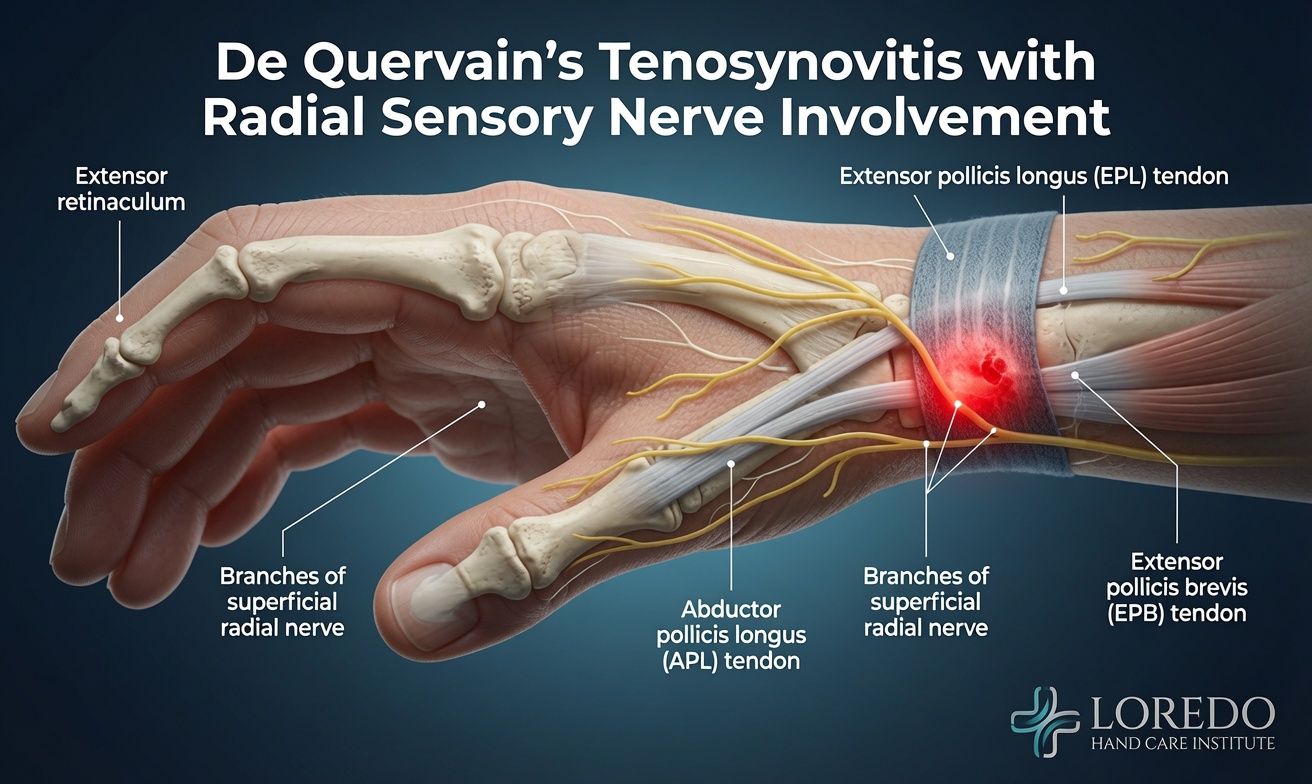
The first dorsal compartment is one of six fibrous tunnels at the dorsal wrist that hold the wrist and finger extensor tendons in place. The first compartment specifically contains two tendons that move the thumb: the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB). When these tendons or their surrounding sheath thicken, the tendons no longer glide smoothly through the compartment. The result is De Quervain's tenosynovitis: pain at the radial wrist that worsens with thumb motion or with ulnar deviation of the wrist.
Surgical release divides the retinaculum overlying the compartment, immediately decompressing the tendons. A critical anatomic detail is that in 60 to 80 percent of patients the compartment is divided by an internal septum into two sub-compartments: one containing the APL and one containing the EPB. Both sub-sheaths must be released for the surgery to succeed. Missing the EPB sub-sheath is the most common cause of persistent symptoms after De Quervain's release. For full background on the underlying condition, see De Quervain's Tendonitis.
Who Is a Candidate?
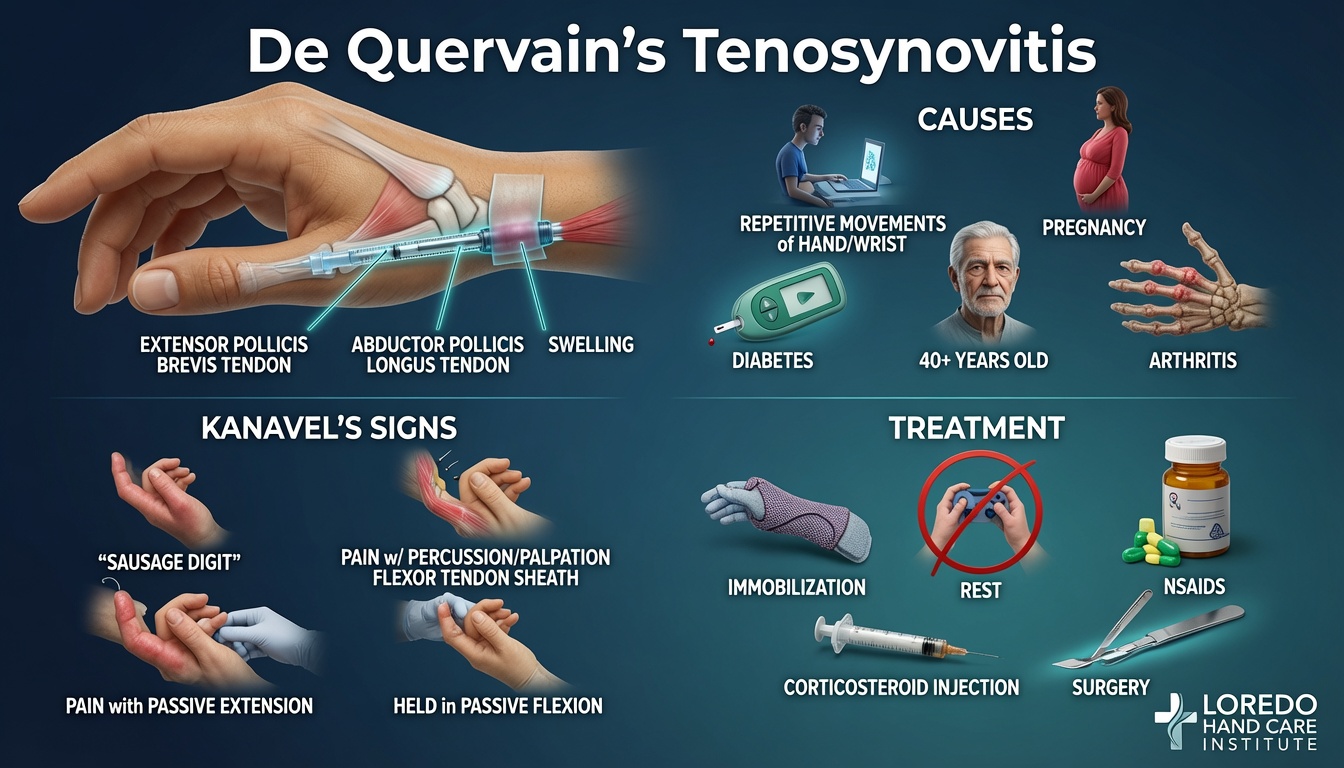
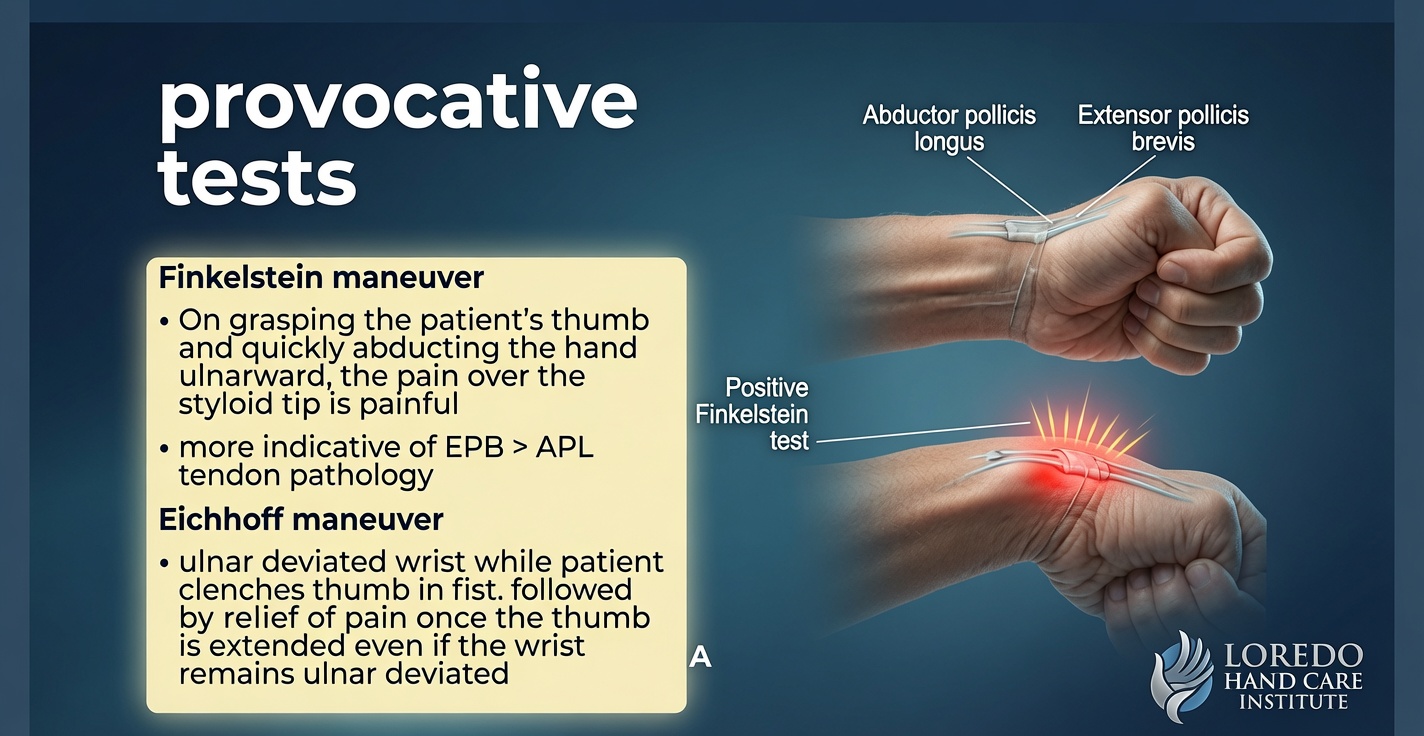
- De Quervain's tenosynovitis confirmed by clinical examination, with positive Finkelstein or Eichhoff testing
- Failure of 6 to 12 weeks of thumb spica splinting and activity modification
- Failure of 1 to 2 corticosteroid injection trials, or recurrence within 3 to 6 months of injection
- Severe symptoms that prevent participation in conservative therapy or interfere with infant care in postpartum patients
- Coexistence with thumb CMC arthritis where conservative care has failed

How the Procedure Is Performed
- Positioning and anesthesia. The patient is supine with the affected arm extended on a hand table. The radial wrist is prepped and draped. Local anesthetic is injected at the surgical site.
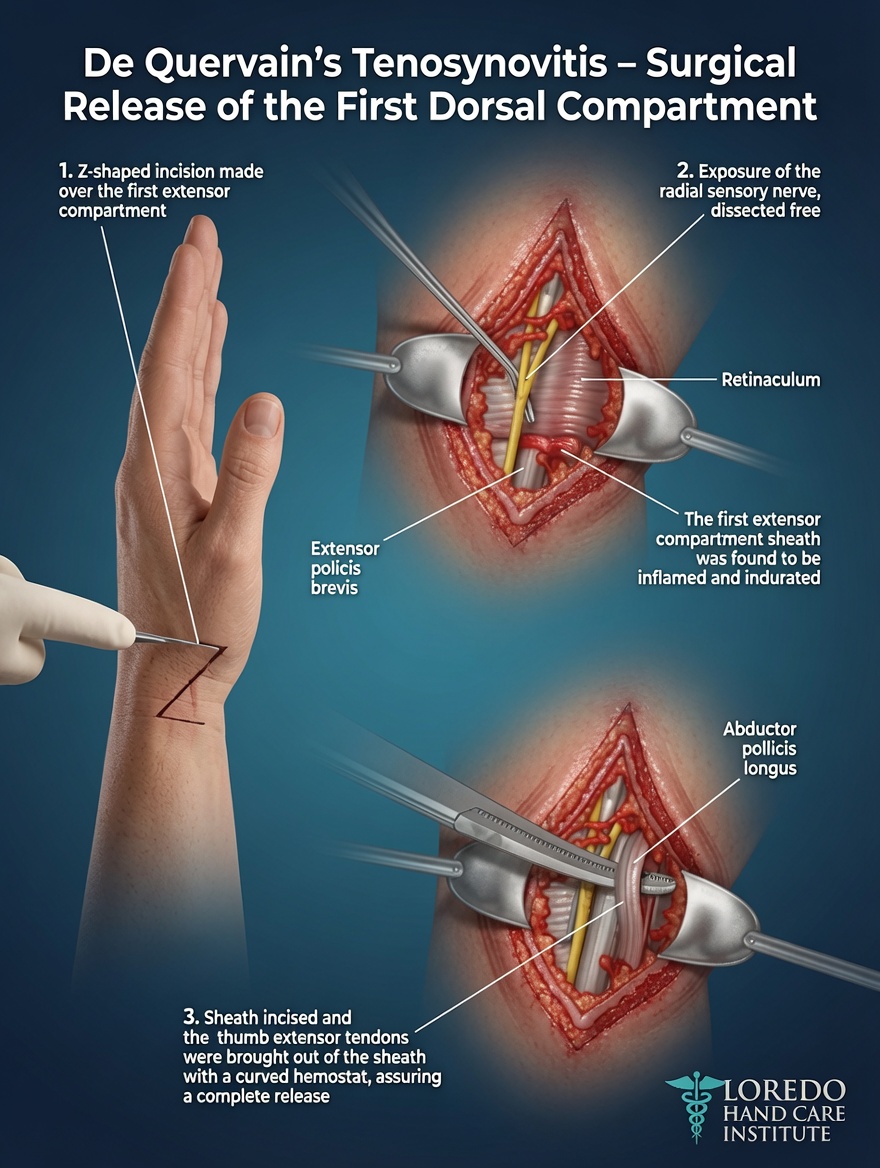
- Incision. A small transverse incision (1.5 to 2 cm) is made directly over the first dorsal compartment at the radial styloid, in the natural skin crease for cosmetic results.
- Nerve identification. The branches of the superficial radial nerve are identified and gently retracted. This is the key technical step: the nerve is found and protected before any tendon-related dissection.
- Retinaculum release. The retinaculum overlying the first compartment is divided longitudinally along the entire length of the compartment.
- Sub-sheath identification and release. The APL and EPB tendons are inspected. Any internal septum dividing them into sub-compartments is identified and released. In 60 to 80 percent of patients, a separate EPB sub-sheath is found and divided.
- Tendon glide test. The patient (awake) actively moves the thumb to confirm smooth tendon gliding through the released compartment.
- Closure. Skin is closed with a fine absorbable suture or adhesive strips. Soft dressing is applied.
Anesthesia Options
- Local anesthesia only (standard): the wrist is numbed with local anesthetic. No sedation is needed. Patients are fully awake and can confirm tendon glide at the end of the procedure.
- Local plus light sedation: available on request for high-anxiety patients.
- Wide-awake local anesthesia (WALANT): with epinephrine in the local anesthetic, allowing tourniquet-free surgery.
Procedure Duration and Setting
The actual surgical time is 15 to 30 minutes. Total time at the office surgical suite or surgery center is 45 to 90 minutes including check-in, anesthetic, the procedure, and a brief recovery. Either setting is appropriate. The procedure can be performed in the office for most patients, which has lower facility fees and a shorter total visit.
Recovery Timeline
- Day 0 to 2: Light hand use after the local wears off. Most patients are off pain medication by day 2.
- Day 2 to 7: Most patients return to typing and light desk work. Postpartum patients can lift and carry the baby with the unaffected hand and gradually with the operated hand.
- Week 1: First post-operative visit; dressing removed. No skin sutures to remove.
- Week 2 to 4: Full activity returns including manual labor and full infant care.
- Week 4 to 8: Scar softens. Mild residual tenderness at the incision typically resolves within 6 to 8 weeks.

Return to Work and Daily Activities
- Office or desk work: 2 to 5 days
- Light manual labor and full infant care: 2 to 4 weeks
- Heavy manual labor and forceful gripping: 4 to 6 weeks
- Driving: within 1 to 2 days for most patients (local-only anesthesia)
Why a Careful Technique Matters
- Identification of the superficial radial nerve before any release prevents the most common complication: numbness in a patch of dorsal thumb skin.
- Release of every sub-sheath, including the EPB sub-sheath in 60 to 80 percent of patients, ensures complete decompression and prevents persistent symptoms.
- Active glide test at the end of the procedure confirms a complete release before closure.
- Small transverse incision in the skin crease minimizes scar visibility.
- Local anesthesia only avoids sedation, fasting, and the need for a driver.
Risks and Complications
- Superficial radial nerve injury: the most recognized complication. Numbness in a patch of dorsal thumb skin. Risk minimized by careful identification and protection of the nerve before any release. Resolves over weeks to months in most cases.
- Incomplete release with persistent EPB symptoms: from a missed EPB sub-sheath. Avoided by routine inspection for sub-compartments.
- Tendon subluxation: rare; the tendons can shift volarly when the retinaculum is released too aggressively. Treated with revision in selected cases.
- Infection (less than 1 percent): treated with antibiotics.
- Scar tenderness: typical; resolves over weeks.
- Persistent symptoms: uncommon when the surgery is complete.
Cost and Insurance
De Quervain's release (CPT 25000) is covered by virtually all commercial insurance plans, Medicare, the VA Community Care Network, and Texas workers' compensation when the diagnosis is appropriately documented. Office-based surgery typically has lower facility fees than ASC procedures. Our team verifies your benefits before surgery. Call our office at (972) 939-4974 for a benefits check.
Frequently Asked Questions
Why do all sub-sheaths need to be released?
In 60 to 80 percent of patients, the first dorsal compartment is divided by an internal septum into two separate sub-compartments: one containing the abductor pollicis longus (APL) and one containing the extensor pollicis brevis (EPB). If the surgeon releases only the main retinaculum and misses the EPB sub-sheath, the EPB tendon remains compressed and symptoms persist. Identifying and releasing every sub-sheath is the single most important technical detail that determines whether the surgery succeeds. This is why a fellowship-trained hand surgeon, who knows to look specifically for the sub-sheath, has higher success rates than less experienced surgeons.
What is the risk to the superficial radial nerve?
The superficial radial nerve runs directly across the surgical area in the dorsal radial wrist. Branches of this nerve must be identified and protected during the procedure. Inadvertent injury produces numbness in a patch of skin on the dorsal thumb and is the most common complication of De Quervain's release in less experienced hands. With careful technique by a fellowship-trained hand surgeon, nerve injury is uncommon. We routinely identify and tag the nerve before any release is performed.
Is this an office procedure or a surgery center procedure?
De Quervain's release can be performed in either an office surgical suite or an ambulatory surgery center, depending on patient factors and insurance authorization. The procedure itself is the same. Office-based surgery typically has a lower facility fee and a shorter total visit time. Surgery center procedures may be required by some insurance plans or for patients who prefer light sedation in addition to local anesthetic. Either setting produces the same outcome.
How long is recovery?
Recovery is short. Most patients use the hand for light tasks within 1 to 2 days. Office or desk work resumes within a few days. Full activity, including manual labor and infant care, returns within 2 to 4 weeks. Hand therapy is not needed for most patients. Postpartum patients with mommy thumb often see immediate symptom relief because the procedure directly addresses the constriction.
Will I need to stop breastfeeding?
No. The procedure uses local anesthetic only and does not require systemic medications that affect breastmilk. Postpartum patients can continue breastfeeding without interruption. The wound is small enough that infant handling resumes within 1 to 2 days. Some patients prefer to take an oral pain medication for the first night, in which case we coordinate with the pediatrician on the appropriate choice and timing relative to feeds.
Related Conditions
- De Quervain's Tendonitis: the underlying condition this procedure treats.
- Pregnancy Hand Pain: postpartum De Quervain's (mommy thumb), the most common pattern in young women.
- Wrist Tendonitis: De Quervain's is the first dorsal compartment subtype; other compartments may also be involved in some patients.
- Thumb Basilar Joint Arthritis: thumb-side wrist condition that can coexist with De Quervain's and is differentiated by examination and selective injection.
Related Procedures
- Open A1 Pulley Release for Trigger Finger: another office-based hand procedure with a similar local-anesthesia approach.
- Endoscopic Carpal Tunnel Release: combined with De Quervain's release in postpartum patients with both conditions.
- CMC Reconstruction: occasionally combined with De Quervain's release when both conditions are present.
- All Procedures: the full list of surgical procedures offered at the practice.
From the Blog
- De Quervain Release Recovery Guide: post-op week-by-week timeline.
- Intersection Syndrome vs De Quervain: ruling out the more proximal mimic.
Watch: De Quervain's release education
Short videos from Dr. Loredo's Instagram and Facebook channels.