Wrist tendonitis is inflammation of one or more of the tendons that cross the wrist. The dorsal (back) wrist contains six anatomic compartments housing the extensor tendons. The volar (front) wrist contains the FCR, FCU, and palmaris longus. Each tendon can become inflamed, producing a localized pattern of pain, tenderness, and pain with resisted motion. The most common patterns are ECU tendonitis (compartment VI), De Quervain's (compartment I, covered on a dedicated page), intersection syndrome (where the first and second compartment tendons cross on the dorsal forearm), FCR tendonitis on the radial volar wrist, and FCU tendonitis on the ulnar volar wrist. Most cases respond to rest, splinting, anti-inflammatory medication, and selective corticosteroid injection.
The Anatomy of the Wrist Tendons
The wrist contains tendons that cross from the forearm muscles to insertions in the hand. They are organized into anatomic compartments held in place by retinacular bands at the wrist.
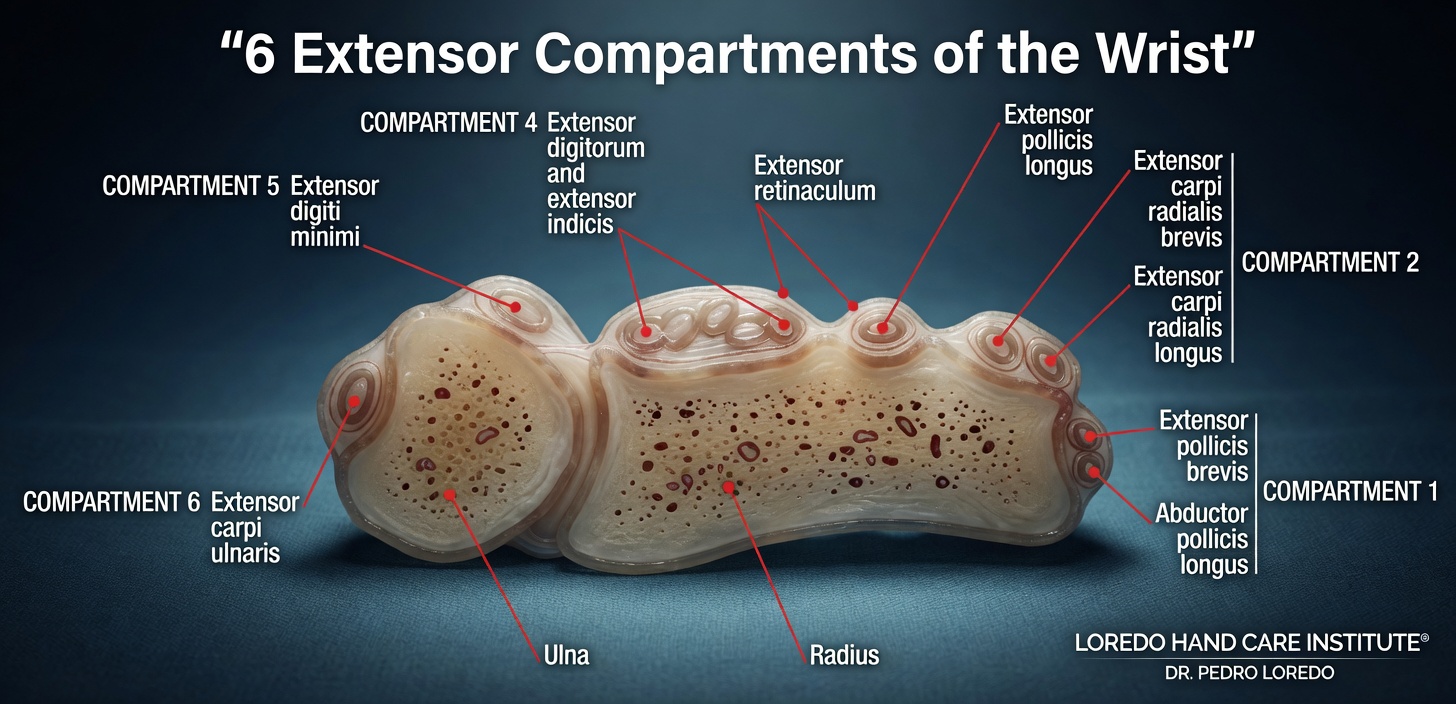
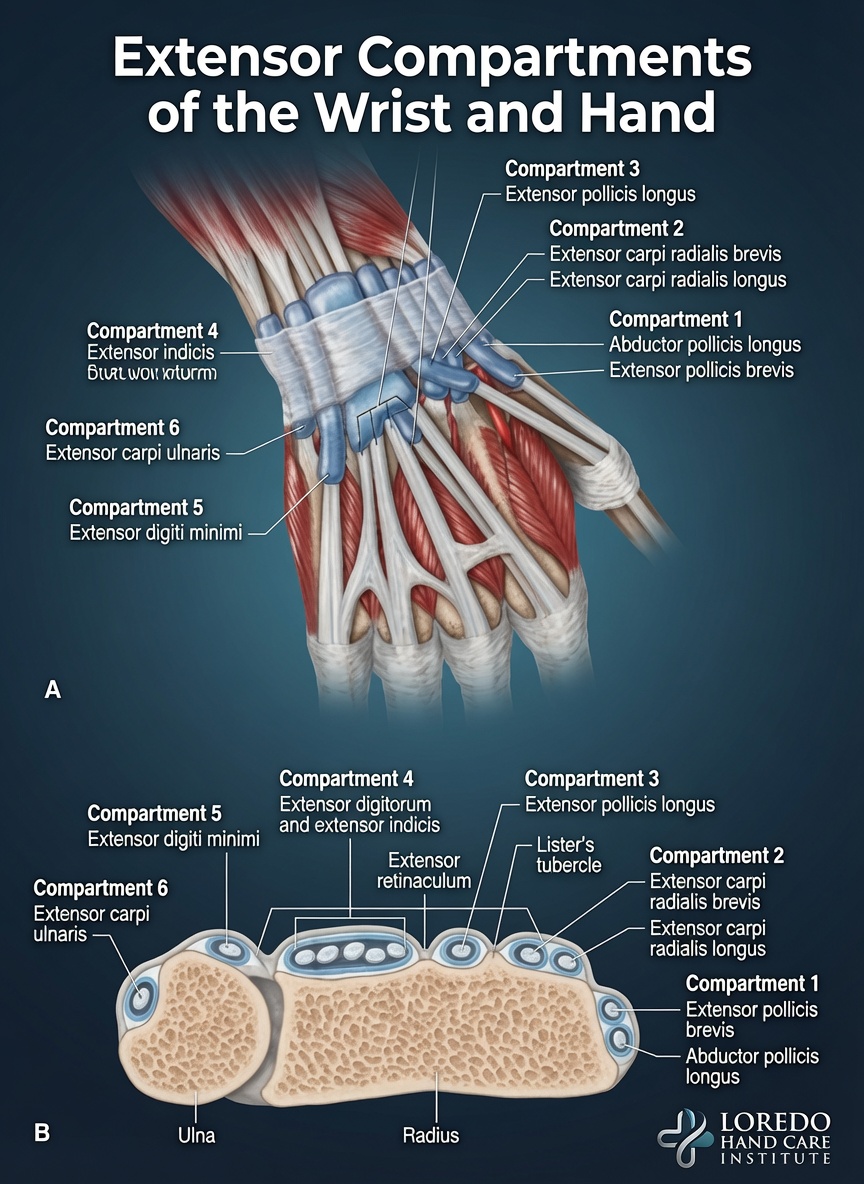
The dorsal (back) wrist contains six compartments under the extensor retinaculum, numbered from radial (thumb side) to ulnar (small finger side):
- Compartment I: Abductor pollicis longus (APL) and extensor pollicis brevis (EPB). The De Quervain's compartment.
- Compartment II: Extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB).
- Compartment III: Extensor pollicis longus (EPL), which curves around Lister's tubercle.
- Compartment IV: Extensor digitorum communis (EDC) and extensor indicis proprius (EIP).
- Compartment V: Extensor digiti minimi (EDM).
- Compartment VI: Extensor carpi ulnaris (ECU), held in its own subsheath that is intimate with the TFCC.
The volar (front) wrist contains the flexor carpi radialis (FCR), flexor carpi ulnaris (FCU), palmaris longus (PL, absent in 15 percent of people), and the long finger flexors that pass through the carpal tunnel.
Clinical coding: ICD-10 M65.831 (right wrist), M65.832 (left wrist). SNOMED CT 25979001.
Common Tendonitis Patterns
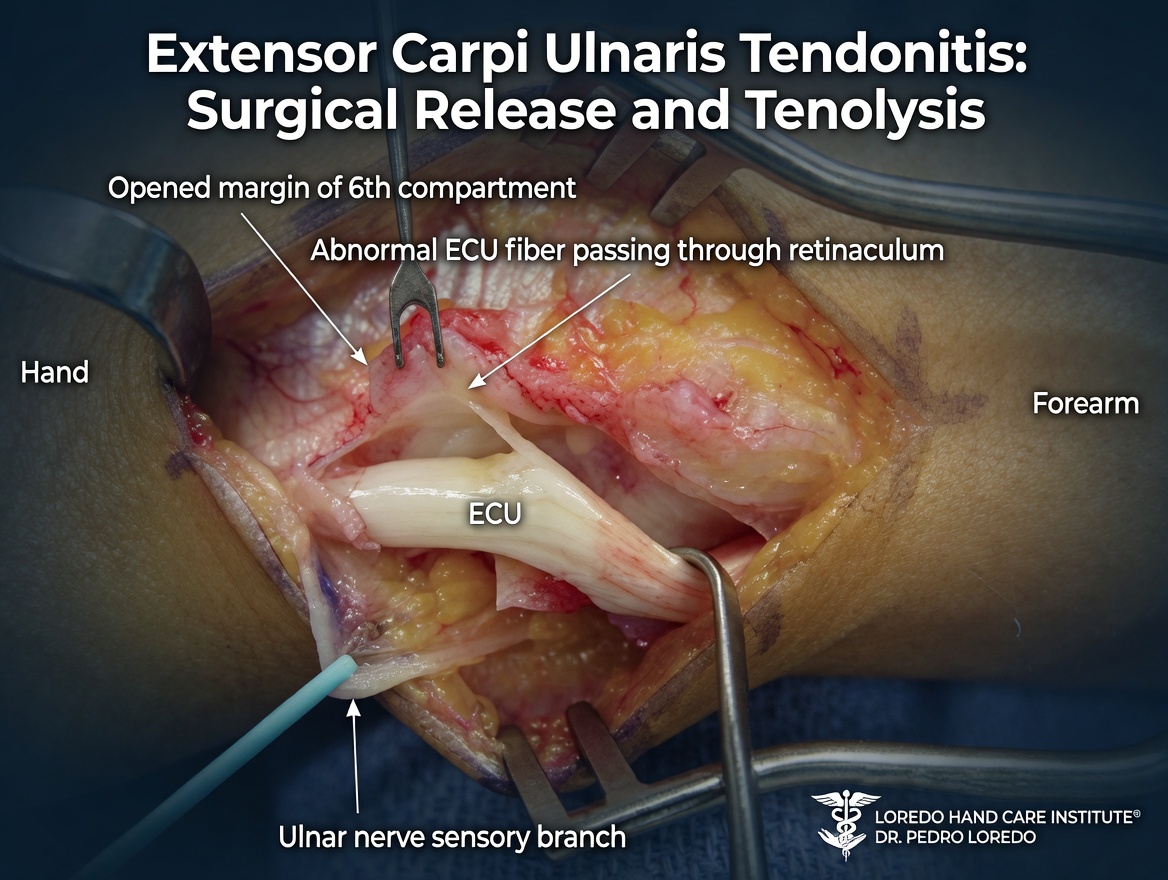
ECU Tendonitis (Compartment VI)
The most common dorsal tendonitis after De Quervain's. Pain on the ulnar dorsal side of the wrist, worse with forearm rotation and ulnar deviation. Often associated with golf, racquet sports, and any activity that loads the ulnar wrist in supination. ECU subluxation, in which the tendon snaps in and out of its subsheath, is a related condition.

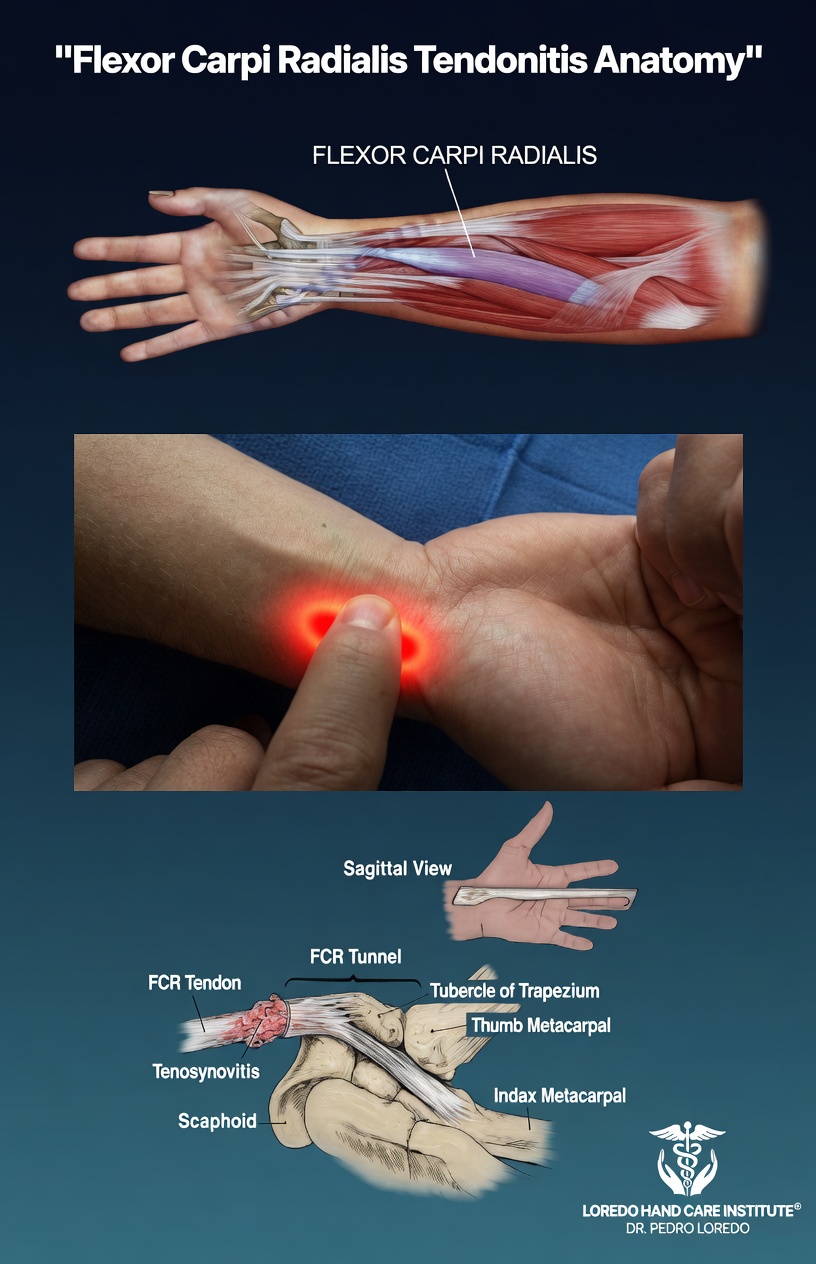
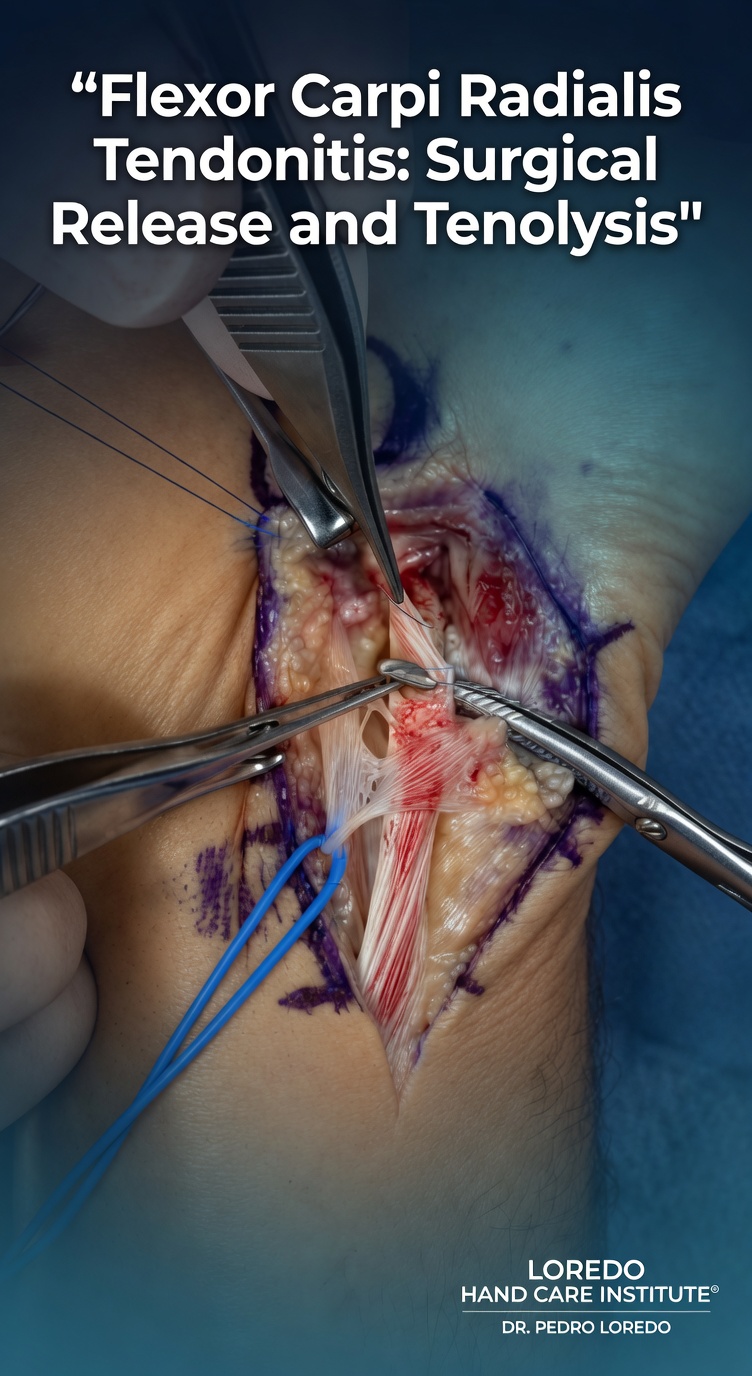
FCR Tendonitis
Pain on the radial volar side of the wrist along the FCR tendon, often where it passes through a fibro-osseous tunnel near the trapezium. Associated with weight training, gripping, and wrist flexion against load. Sometimes coexists with thumb CMC arthritis because of the proximity of the tendon to the joint.
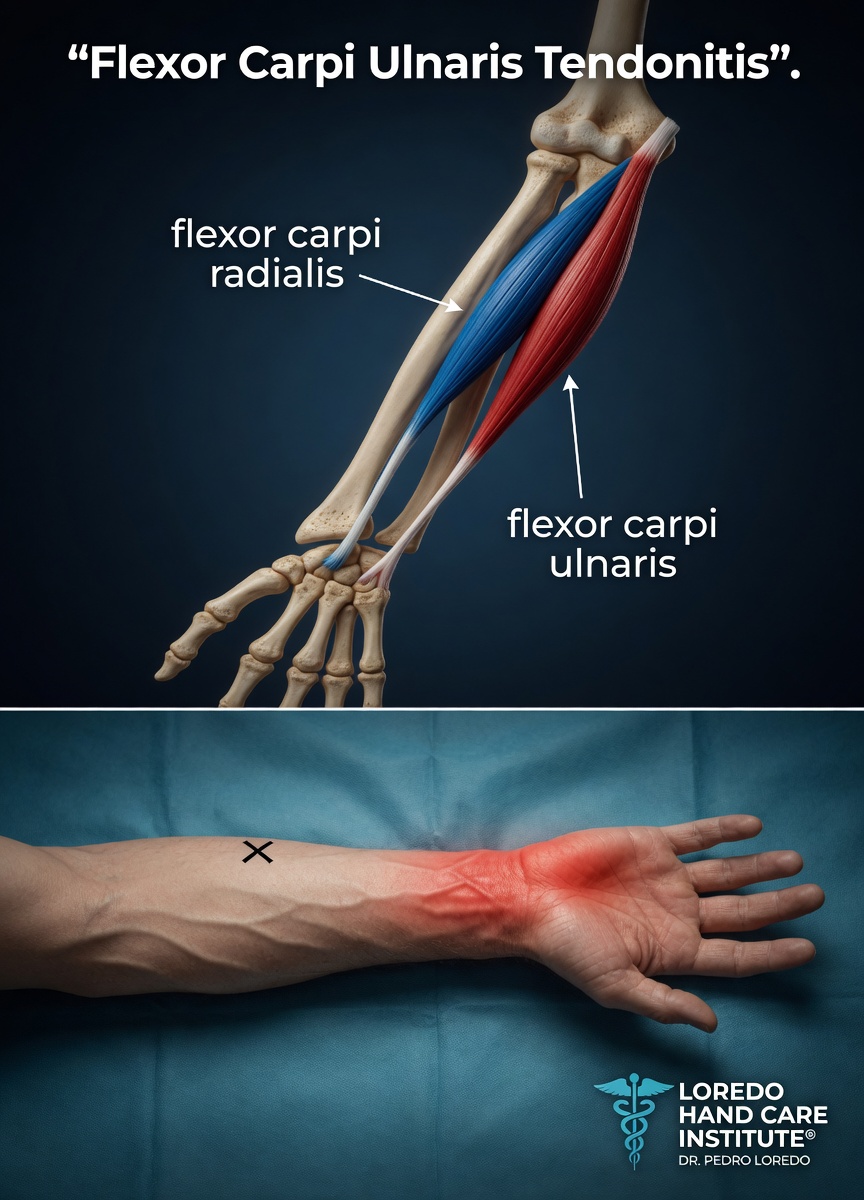
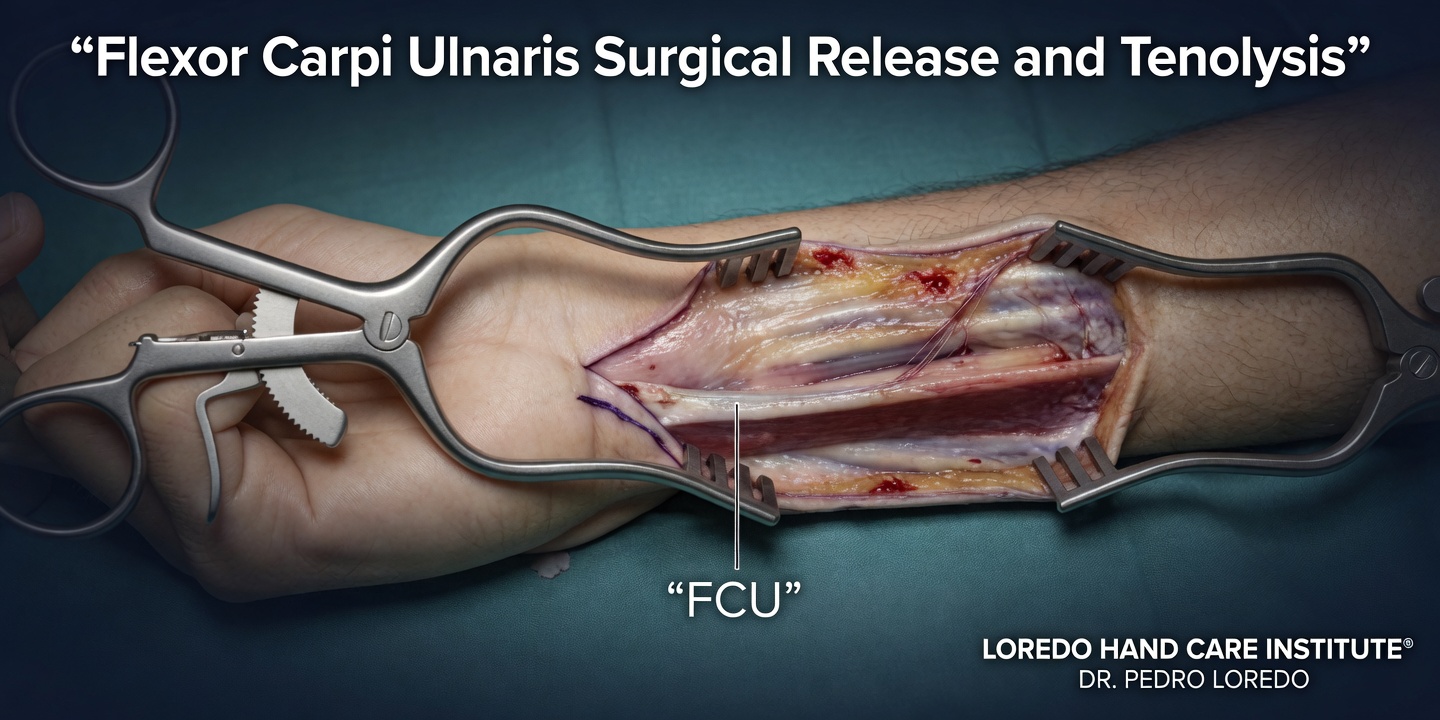
FCU Tendonitis
Pain on the ulnar volar wrist where the FCU inserts on the pisiform. Tenderness localizes directly over the pisiform bone. Repetitive wrist flexion under load, including weight training and rock climbing, is the typical trigger.
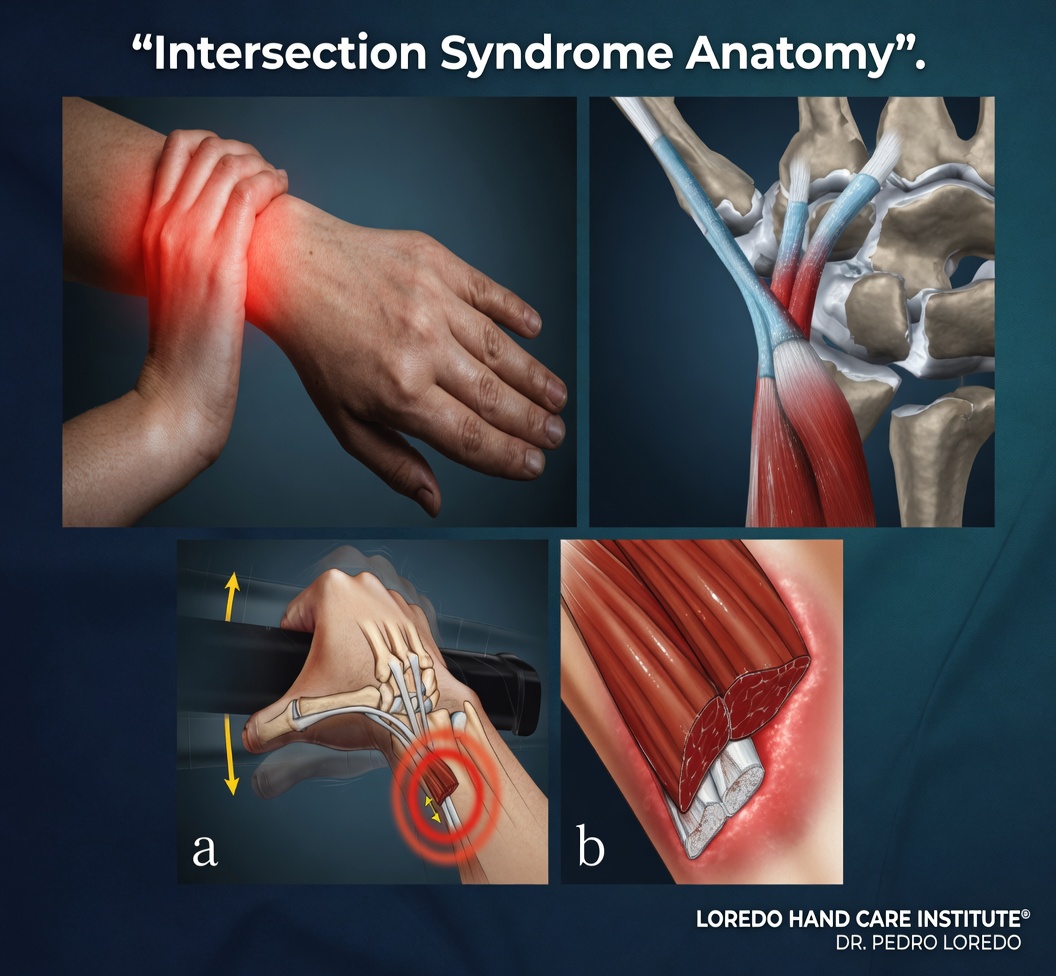
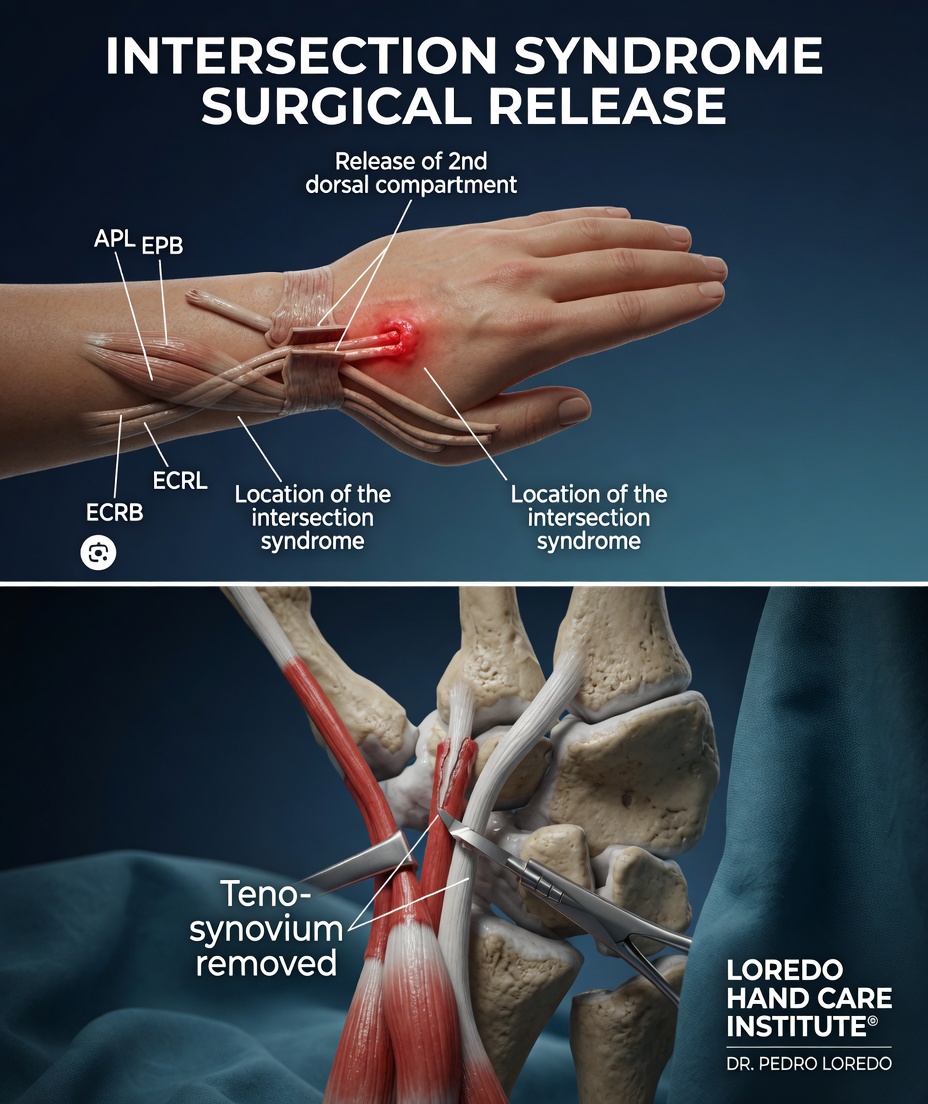
Intersection Syndrome
Pain about 4 to 6 cm proximal to the wrist on the dorsal radial forearm at the point where the first compartment tendons cross over the second compartment tendons. Crepitus (a creaking or squeaking sound with motion) and visible swelling are characteristic. Common in rowers, weightlifters, and others with repetitive wrist extension under load.
EPL Tendonitis and Rupture
Inflammation of the EPL tendon as it curves around Lister's tubercle in the third compartment. Pain on the dorsal radial wrist that worsens with thumb extension. Notable because the tendon is at risk for spontaneous rupture, particularly after an undisplaced distal radius fracture and in patients with rheumatoid arthritis.
Causes and Risk Factors
- Repetitive wrist motion under load: manual work, weight training, rowing, racquet sports
- Sudden increase in training intensity or starting a new repetitive task
- Direct trauma to the affected compartment
- Poor ergonomics at a workstation
- Pregnancy and postpartum hormonal changes (more common for first compartment tenosynovitis)
- Inflammatory arthritis, particularly rheumatoid disease, which causes chronic synovitis at multiple compartments simultaneously
- Anatomic variants such as a thickened retinaculum or accessory tendon slips
Symptoms and Warning Signs
- Localized pain in a specific area of the wrist
- Tenderness on direct palpation over the affected compartment
- Pain reproduced by resisted motion of the involved tendon
- Swelling along the tendon
- Crepitus or a creaking sound with motion (especially in intersection syndrome)
- Pain that worsens with the activity that produced symptoms
- Stiffness in the morning that loosens with light activity
- Snapping sensation in the case of ECU subluxation
How the Diagnosis Is Made
Diagnosis is clinical. The location of maximal tenderness and the specific maneuver that reproduces pain together identify which compartment is involved.
- Tenderness mapping: the examiner palpates each compartment and tendon to localize the maximum point of tenderness.
- Resisted motion testing: resisted thumb extension, wrist extension, ulnar deviation, radial deviation, and forearm rotation each load specific tendons. Pain reproduction in a specific direction confirms the compartment.
- Finkelstein test (for compartment I): the patient makes a fist over the thumb and ulnarly deviates the wrist. Sharp pain at the radial styloid is positive for De Quervain's.
- ECU synergy test (for compartment VI): with the elbow on the table, palm up, the patient resists thumb radial abduction. ECU tightening reproduces ulnar wrist pain when ECU tendonitis is present.
- Imaging: X-ray rules out wrist arthritis or fracture as a pain source. Ultrasound confirms tendon thickening, tenosynovial fluid, and ECU subluxation. MRI is selectively used for chronic or atypical cases.
Non-Surgical Treatment Options

- Rest from the aggravating activity for 1 to 4 weeks depending on severity
- Wrist splint in a neutral position to immobilize the affected compartment, worn during aggravating tasks and at night
- Topical and oral nonsteroidal anti-inflammatory medication for symptom relief
- Ice over the affected area 15 to 20 minutes several times per day
- Targeted hand therapy with stretching, friction massage, and progressive strengthening once acute symptoms settle
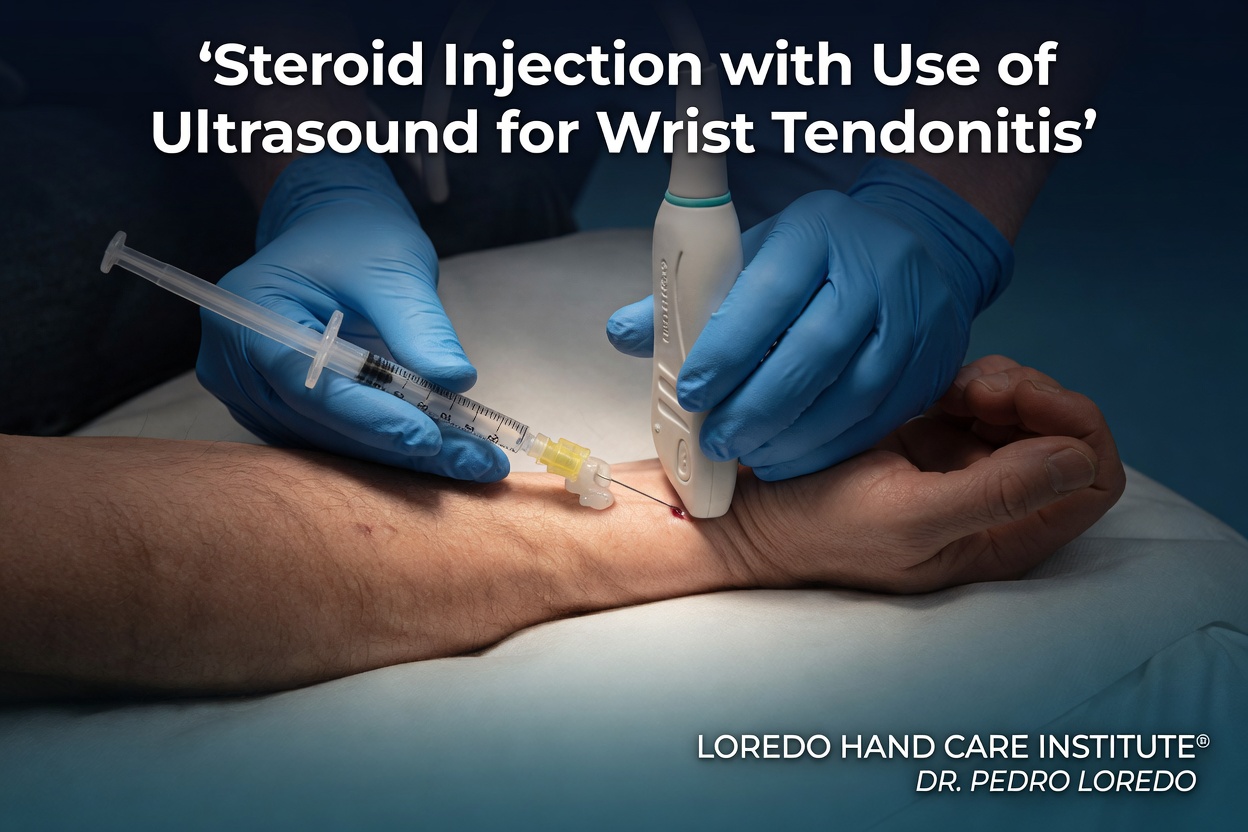
- Targeted corticosteroid injection into the affected compartment under ultrasound guidance for moderate-to-severe symptoms or when conservative measures have failed
- Workstation ergonomic assessment to identify and modify the loading pattern that caused symptoms
The great majority of wrist tendonitis cases resolve within 4 to 8 weeks with appropriate conservative care.
Surgical Options
Surgery is uncommon for most wrist tendonitis patterns. It is considered when conservative care including injection has failed for 3 to 6 months and symptoms continue to limit work or daily activity.
Compartment Decompression
Release of the retinaculum overlying the affected compartment to relieve pressure. Most commonly performed for refractory De Quervain's (covered on the dedicated De Quervain's page), occasionally for refractory ECU tendonitis, and rarely for the other compartments.
ECU Subsheath Reconstruction
Recurrent ECU subluxation that is symptomatic despite conservative treatment may require reconstruction of the subsheath to stabilize the tendon in its groove.
EPL Reconstruction
EPL rupture, particularly after distal radius fracture, is treated with EIP tendon transfer to restore thumb extension. The procedure has reliable functional results.
Recovery Timeline
- Mild conservative cases: symptoms improve within 1 to 2 weeks of rest and splinting.
- Moderate to severe conservative cases: 4 to 8 weeks of structured care.
- Patients receiving corticosteroid injection: substantial relief within 24 to 72 hours, with continued improvement over 2 to 4 weeks.
- Surgical decompression: 4 to 6 weeks of dressing and splint care, then progressive return to activity over 8 to 12 weeks.
- EPL transfer: 4 weeks of immobilization, then 4 to 8 weeks of structured therapy.
- Return to repetitive manual work or sport requires progressive strengthening to prevent recurrence.
Returning to Work and Daily Activity
- Office or desk work: within days for most patients
- Light manual labor: 2 to 4 weeks for conservative cases; 6 to 8 weeks after surgery
- Heavy manual labor: 6 to 8 weeks for conservative cases; 10 to 12 weeks after surgery
- Sport that loads the wrist: 6 to 12 weeks with attention to technique and load progression
Frequently Asked Questions
What are the six dorsal compartments?
The six dorsal compartments are anatomic tunnels under the extensor retinaculum at the back of the wrist. From thumb to small finger they are: I (APL and EPB, the De Quervain's compartment), II (ECRL and ECRB), III (EPL around Lister's tubercle), IV (EDC and EIP), V (EDM), and VI (ECU, on the ulnar side of the wrist). Each compartment can develop tenosynovitis, which produces localized pain, tenderness, and pain with resisted motion of the tendons it contains.
Is this the same as De Quervain's tendonitis?
De Quervain's tendonitis is a specific type of wrist tendonitis affecting the first dorsal compartment (APL and EPB). It is so common that it has its own dedicated condition page. Other wrist tendonitis patterns affect different tendons in different locations: ECU tendonitis on the ulnar dorsal side, FCR or FCU tendonitis on the volar side, intersection syndrome at the junction of compartments I and II, and EPL tendonitis around Lister's tubercle. Each pattern has its own location-specific tenderness and treatment.
What is intersection syndrome?
Intersection syndrome is tendonitis at the point on the dorsal forearm, about 4 to 6 cm proximal to the wrist, where the tendons of the first dorsal compartment (APL and EPB) cross over the tendons of the second dorsal compartment (ECRL and ECRB). The friction between the crossing tendons produces a localized swelling, crepitus (a creaking or squeaking sound with motion), and pain. Treatment is the same as for other compartment tendonitis: rest, splinting, NSAIDs, and selective corticosteroid injection.
Do I need cortisone or surgery for wrist tendonitis?
Most cases of wrist tendonitis resolve with rest, activity modification, splinting, and anti-inflammatory medication over 4 to 8 weeks. A targeted corticosteroid injection into the affected compartment is appropriate when conservative measures fail or when the patient has severe symptoms that prevent participation in therapy. Surgical decompression of the compartment is reserved for cases that do not respond to a structured course of conservative care including injection, and is uncommon for most wrist tendonitis patterns outside of De Quervain's.
How long until I can return to my normal activities?
Mild cases improve within 1 to 2 weeks of activity modification and splinting. Moderate to severe cases typically take 4 to 8 weeks of structured conservative care. Patients who receive a corticosteroid injection often see substantial relief within days. Return to repetitive manual work or sport requires an additional 2 to 4 weeks of progressive strengthening to prevent recurrence. Recurrent tendonitis is common in patients who return to the same loading pattern that produced symptoms without addressing technique or workload.
When to Call the Doctor
Call our office for evaluation if you experience:
- Localized wrist pain that has lasted more than a few weeks
- Pain that worsens with specific motions or specific activities
- Visible swelling or a creaking sensation along a tendon
- Failure to improve with rest, splinting, and anti-inflammatory medication
- A snapping sensation on the ulnar side of the wrist with rotation (suspect ECU subluxation)
- Sudden inability to extend the thumb tip after a healed wrist fracture (suspect EPL rupture)
- Recurrent tendonitis after a previous successful treatment
After surgery, call promptly if you experience fever over 101°F, expanding redness or drainage at the incision, severe pain not controlled by medication, or a sudden new motion deficit.
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- De Quervain's Tendonitis: the most common wrist tendonitis pattern. Affects the first dorsal compartment specifically and has its own dedicated page.
- Trigger Finger: a related but distinct tendinopathy at the A1 pulley. Often coexists in patients with diabetes and inflammatory arthritis.
- TFCC Tears: ulnar wrist pain that overlaps clinically with ECU tendonitis. The TFCC and the ECU subsheath are anatomically intimate and both can be involved in ulnar wrist pain.
- Hand and Wrist Arthritis: chronic synovitis of inflammatory arthritis affects multiple wrist compartments simultaneously and can produce a multifocal tendonitis pattern.
- Hand and Finger Fractures: EPL rupture is a recognized late complication of distal radius fractures and can produce sudden loss of thumb extension.
From the Blog
- Intersection Syndrome vs De Quervain: two wrist tendinopathies anatomically distinct.
- Ergonomic Tips for Hand Pain: wrist-position and grip-technique changes.
- When a Cortisone Injection Is the Right Choice: response patterns for wrist tendinopathy.
Watch: Wrist tendonitis education
Short videos from Dr. Loredo's YouTube and Facebook channels.