TFCC tears are injuries to the triangular fibrocartilage complex, a wedge of cartilage and ligaments on the ulnar (small finger) side of the wrist that cushions load and stabilizes the distal radioulnar joint. Tears occur from a single traumatic event such as a fall on an outstretched hand, from a forceful twisting injury, or gradually from chronic load when the ulna is slightly longer than the radius (ulnar-positive variance). Patients present with ulnar-sided wrist pain that is worse with forearm rotation, gripping, and load. The Palmer classification separates traumatic from degenerative tears and guides treatment, which ranges from immobilization and corticosteroid injection to arthroscopic debridement or repair, with ulnar shortening osteotomy reserved for ulnar-positive variance with peripheral tearing.
The Anatomy of the TFCC
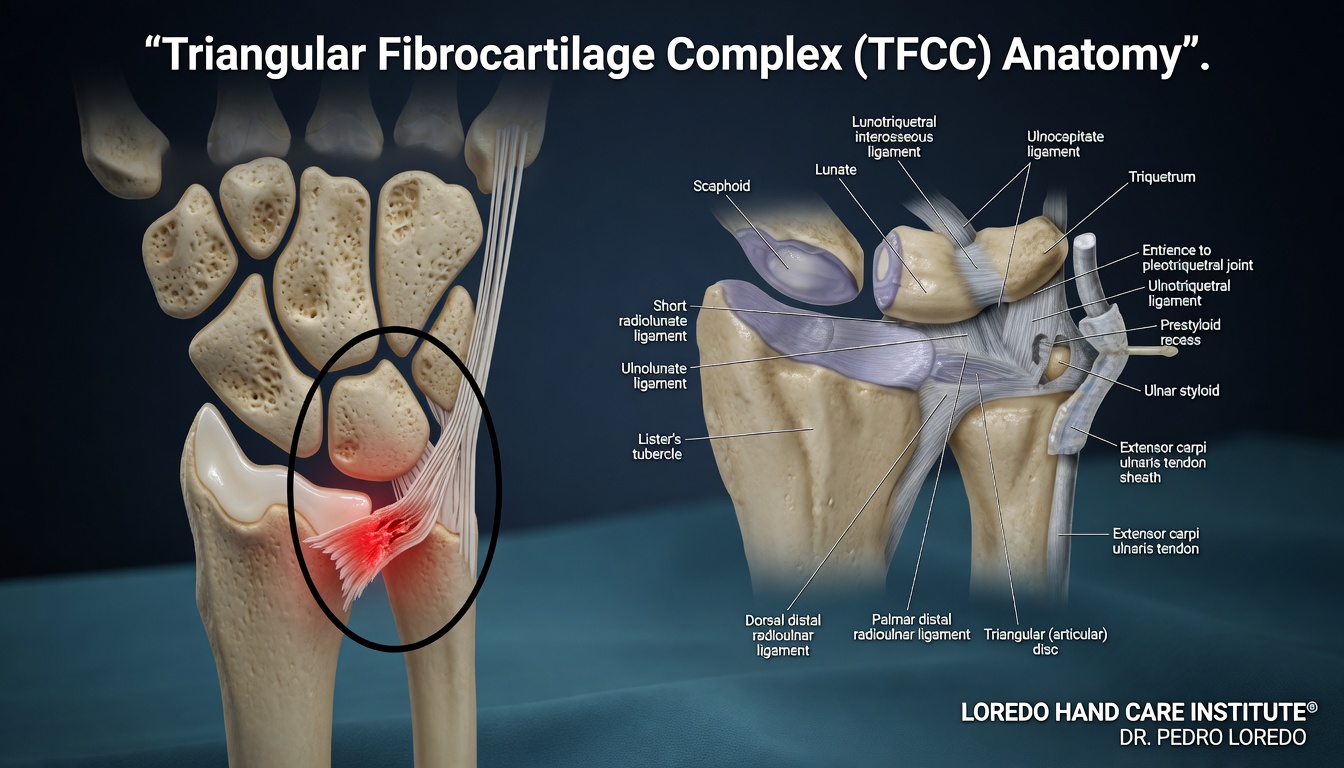
The triangular fibrocartilage complex sits between the distal ulna and the lunate and triquetrum carpal bones. It is shaped like a wedge with the apex at the radius and the base at the ulnar styloid. The complex includes the central articular disc (a fibrocartilage cushion), the dorsal and volar radioulnar ligaments (which stabilize the DRUJ), the ulnocarpal ligaments (the ulnolunate and ulnotriquetral), and the ECU subsheath. The complex serves three functions: it cushions load between the ulnar wrist and the carpus, it stabilizes the DRUJ during forearm rotation, and it carries about 20 percent of the load across the wrist.
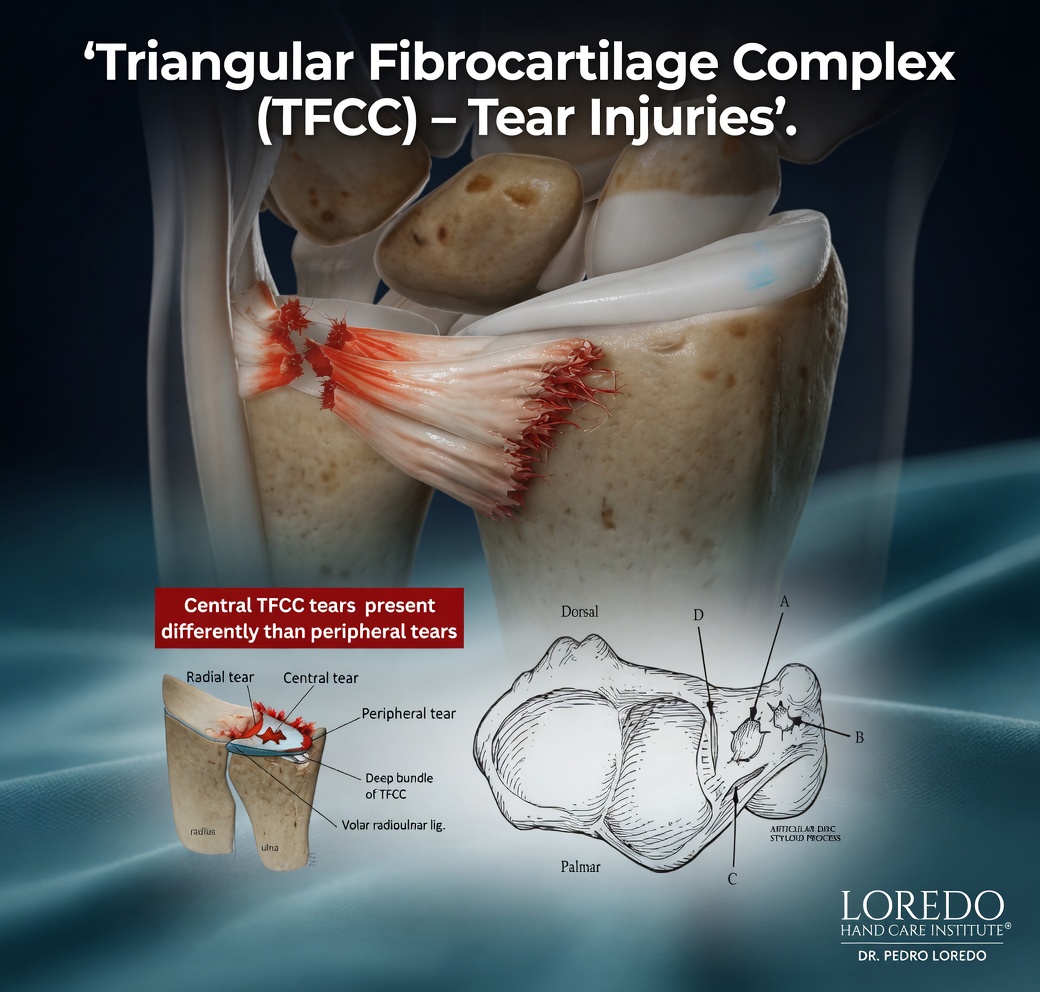
The central portion of the articular disc has poor blood supply and limited capacity to heal. The peripheral portions, particularly the ulnar attachment at the fovea, have a robust blood supply and can heal with appropriate repair. This blood supply pattern is why central tears are typically debrided while peripheral tears can be repaired.
Ulnar variance describes the relative length of the ulna compared to the radius at the wrist. Ulnar-positive variance (ulna longer than radius by more than 2 mm) increases load across the TFCC and predisposes to degenerative tearing. Ulnar-negative variance is associated with Kienbock's disease but rarely with TFCC pathology.
Clinical coding: ICD-10 S63.591A (acute traumatic tear, right wrist), M24.139 (degenerative TFCC tear). SNOMED CT 261011007.
Causes and Risk Factors
- Fall on an outstretched hand, particularly with the forearm pronated
- Forceful twisting injury: a torque wrench slipping, a martial arts joint lock, a rotational fall on a ski pole
- Distal radius fracture: 50 percent or more of distal radius fractures have an associated TFCC tear
- Repetitive load with rotation: mechanics, plumbers, racket sports, gymnastics, weightlifting
- Ulnar-positive variance, congenital or acquired after a malunited distal radius fracture
- Age over 50 for degenerative tears
Symptoms and Warning Signs
- Pain on the ulnar (small finger) side of the wrist, often deep
- Pain that worsens with forearm rotation, especially supination under load
- Pain reproduced by gripping, opening jars, turning a doorknob, or twisting motions
- Tenderness deep in the ulnar fovea (the depression between the ulnar styloid and the FCU tendon)
- Clicking or popping with rotation
- Weakness with twisting or gripping
- Sense of instability at the wrist in advanced cases with associated DRUJ injury
- Symptoms that may follow a discrete injury or develop gradually with overuse
How the Diagnosis Is Made
Diagnosis combines history, examination, imaging, and selective use of wrist arthroscopy as the gold standard.
- Ulnar fovea sign: the most useful single bedside test. Direct pressure on the ulnar fovea (between the ulnar styloid and FCU tendon) reproduces pain in TFCC pathology.
- TFCC compression test: the wrist is ulnarly deviated and axially loaded while rotated. Reproduction of pain is positive.
- Press test: the patient pushes off a chair with the wrists ulnarly deviated. Reproduction of ulnar wrist pain suggests TFCC pathology.
- DRUJ stability assessment: the radius and ulna are translated relative to each other to look for instability that suggests a peripheral TFCC tear.
- X-ray: assesses ulnar variance and looks for distal radius fracture, ulnar styloid fracture, or arthritis.
- MRI or MR arthrogram: shows tears of the TFCC and identifies associated ligament injuries. Sensitivity is approximately 75 to 90 percent for central tears and somewhat lower for peripheral tears.
- Wrist arthroscopy: the gold standard for both diagnosis and treatment. Direct visualization classifies the tear precisely and allows immediate repair or debridement.
Palmer Classification
The Palmer classification organizes TFCC tears by mechanism and location and guides treatment.
- Class 1: Traumatic
- 1A: Central perforation. Avascular zone. Treated with debridement.
- 1B: Ulnar avulsion from the fovea, often with DRUJ instability. Repaired.
- 1C: Distal avulsion of the ulnocarpal ligaments. Repaired.
- 1D: Radial avulsion. Repaired or debrided depending on size.
- Class 2: Degenerative (associated with ulnar-positive variance)
- 2A: TFCC wear without perforation
- 2B: 2A plus chondromalacia of the lunate or ulnar head
- 2C: TFCC perforation with chondromalacia
- 2D: 2C plus lunotriquetral ligament tear
- 2E: Advanced degenerative arthritis
Non-Surgical Treatment Options
- Wrist splint or short arm cast for 4 to 6 weeks for acute traumatic tears without DRUJ instability.
- Activity modification: avoid forceful rotation and gripping for 6 to 12 weeks.
- Topical and oral nonsteroidal anti-inflammatory medication.
- Corticosteroid injection into the ulnar wrist or DRUJ. Both diagnostic and therapeutic. Symptom relief from injection often clarifies whether the TFCC is the pain generator.
- Targeted hand therapy with edema control, range of motion, and progressive strengthening once acute pain settles.
Surgical Options
Surgery is considered for tears that fail conservative care, for tears with DRUJ instability, and for chronic ulnar-positive variance with peripheral tearing.
Arthroscopic Debridement (Class 1A and Class 2 Central Tears)
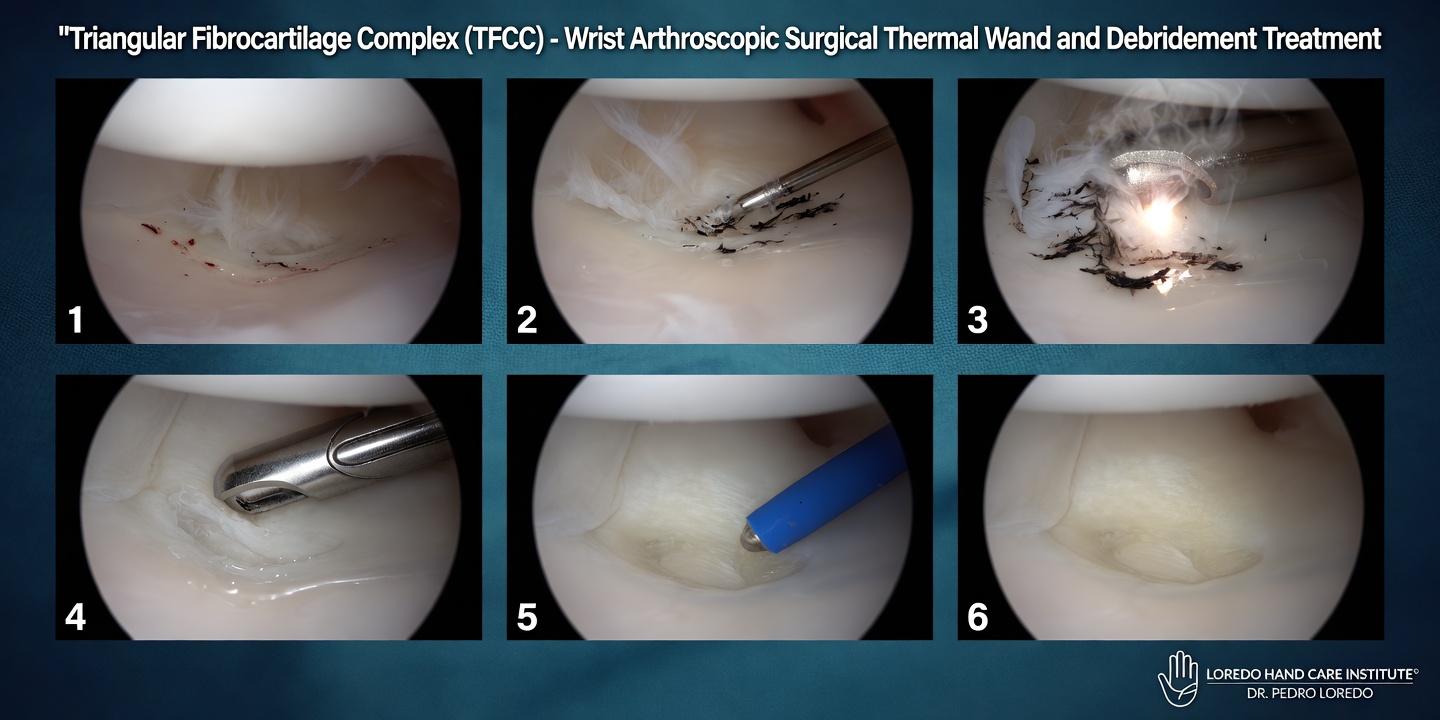
- Outpatient wrist arthroscopy through 2 to 3 small portals
- The torn central portion of the TFCC is shaved smooth with a small motorized shaver
- The peripheral attachment is preserved
- Procedure takes 30 to 45 minutes under regional anesthesia
- Soft dressing and a removable splint for 1 to 2 weeks
Arthroscopic Repair (Class 1B and 1D Peripheral Tears)
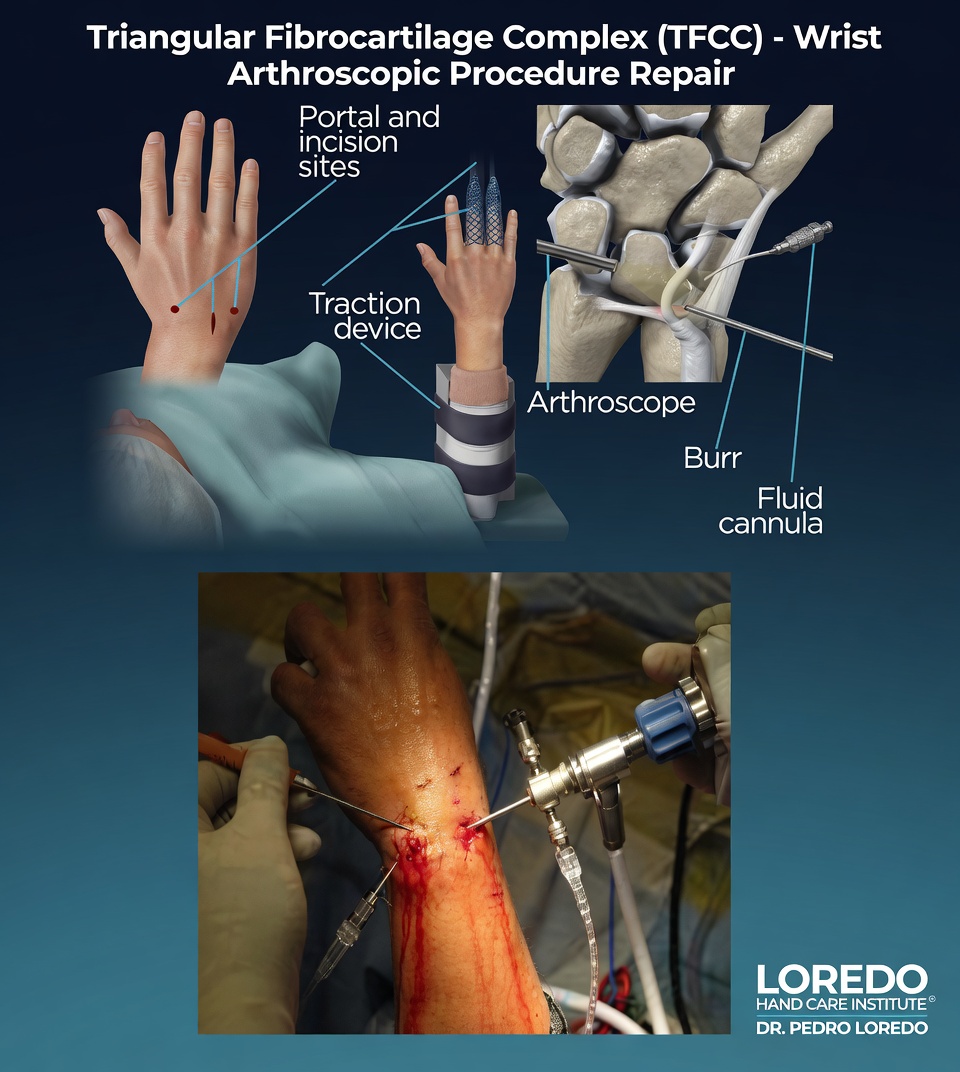
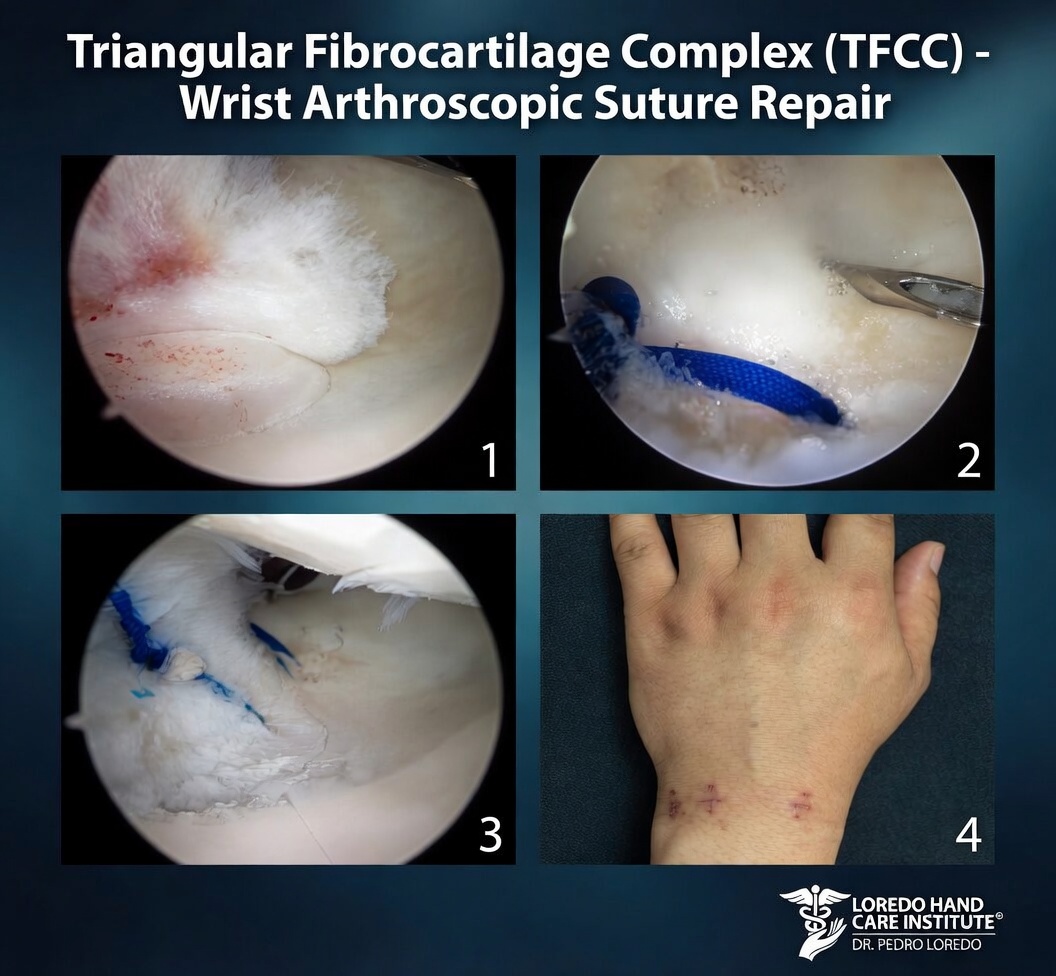
- Outpatient wrist arthroscopy
- The torn peripheral attachment is reattached using outside-in suture passers or suture anchors at the fovea
- A short arm cast or splint for 4 to 6 weeks postoperatively
Ulnar Shortening Osteotomy
- Open procedure for ulnar-positive variance with peripheral TFCC tearing or ulnocarpal impaction
- A 2 to 4 mm wedge of bone is removed from the ulnar shaft and the bone is fixed with a plate
- Reduces load across the TFCC and unloads the ulnar wrist
- Bone healing requires 8 to 12 weeks
Recovery Timeline
- Arthroscopic debridement (Class 1A): Splint 1 to 2 weeks, return to light activity at 2 weeks, full activity at 4 to 6 weeks.
- Arthroscopic repair (Class 1B/D): Cast or splint 4 to 6 weeks, then 4 to 6 weeks of structured hand therapy. Full activity at 3 to 4 months.
- Ulnar shortening osteotomy: Splint 2 weeks, then progressive activity in a removable splint. Bone healing 8 to 12 weeks. Full return at 4 to 6 months.
- Hand therapy is critical to all three procedures and addresses range of motion, edema, scar management, and progressive strengthening.
Returning to Work and Daily Activity
- Office or desk work: 1 to 2 weeks after debridement; 2 to 4 weeks after repair; 2 to 4 weeks after osteotomy
- Light manual labor: 4 to 6 weeks after debridement; 8 to 12 weeks after repair or osteotomy
- Heavy manual labor and load-bearing sport: 8 to 12 weeks after debridement; 4 to 6 months after repair or osteotomy
- Driving: when out of the splint and able to grip the wheel comfortably, usually 1 to 4 weeks
Frequently Asked Questions
What is the TFCC and why does it tear?
The triangular fibrocartilage complex (TFCC) is a wedge of cartilage and ligaments on the ulnar (small finger) side of the wrist. It cushions load between the distal ulna and the carpal bones and stabilizes the joint between the radius and ulna. Tears occur from a single traumatic event such as a fall on an outstretched hand, from a forceful twisting injury (think a torque wrench slipping or a martial arts joint lock), or gradually from chronic load when the ulna is slightly longer than the radius (ulnar-positive variance), which produces wear over years.
How are TFCC tears classified?
The Palmer classification separates traumatic tears (Class 1) from degenerative wear (Class 2). Traumatic tears are graded 1A (central perforation), 1B (ulnar avulsion from the fovea), 1C (distal ulnocarpal ligament avulsion), and 1D (radial avulsion). The location matters because some tears (1A central) heal poorly and are debrided, while others (1B and 1D peripheral) have a blood supply and can be repaired. Degenerative tears (Class 2A through 2E) progress from wear without perforation through cartilage and ligament damage to lunotriquetral instability.
How long should I try conservative treatment first?
At least 6 to 12 weeks of immobilization in a wrist splint or short arm cast, plus activity modification and anti-inflammatory medication, is appropriate for most acute traumatic tears without instability. A corticosteroid injection into the ulnar wrist can be both diagnostic and therapeutic. Surgery is considered for tears that fail conservative care, for tears with associated DRUJ (distal radioulnar joint) instability, and for chronic ulnar-positive variance with peripheral tearing.
Is TFCC repair done arthroscopically?
Yes, in nearly all cases. Wrist arthroscopy uses small portals and a tiny camera to visualize the TFCC directly. Debridement of central tears (Class 1A) is straightforward. Peripheral repair (Class 1B and 1D) is performed with sutures placed through small additional portals or with anchor fixation. Ulnar shortening osteotomy, when needed for ulnar-positive variance, is an open procedure performed alongside or after the arthroscopy.
How long until I can use my hand fully again?
After arthroscopic debridement of a central tear (Class 1A), most patients return to light activity within 2 weeks and full activity within 4 to 6 weeks. After peripheral repair (Class 1B or 1D), the wrist is immobilized for 4 to 6 weeks followed by 4 to 6 weeks of structured hand therapy, with full return to manual work and sport at 3 to 4 months. Ulnar shortening osteotomy requires bone healing and adds 8 to 12 weeks to the recovery, with full activity at 4 to 6 months.
When to Call the Doctor
Call our office for evaluation if you experience:
- Ulnar wrist pain that has lasted more than several weeks
- Pain after a fall on an outstretched hand or a forceful twisting injury
- Pain reproduced by gripping, twisting, or forearm rotation
- Wrist clicking or popping with rotation
- Sense of wrist instability or weakness with twisting tasks
- Persistent ulnar wrist pain after a distal radius fracture has healed
After surgery, call promptly if you experience fever over 101°F, expanding redness or drainage at the incision, severe pain not controlled by medication, or new numbness or weakness in the hand.
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Hand and Finger Fractures: a TFCC tear is associated with up to half of distal radius fractures and is a common cause of persistent wrist pain after the fracture has healed.
- Hand and Wrist Arthritis: chronic untreated TFCC tears with DRUJ instability lead to post-traumatic wrist arthritis. Differentiated from primary arthritis by history and imaging.
- Wrist Tendonitis: ECU tendonitis can produce ulnar-sided wrist pain that overlaps with TFCC pain. The TFCC and the ECU subsheath are anatomically intimate.
- Cubital Tunnel Syndrome: ulnar nerve symptoms occasionally accompany ulnar wrist pain and require separate evaluation.
- Guyon's Canal Syndrome: another ulnar-sided wrist condition. Differentiated by the presence of nerve symptoms (Guyon's) versus mechanical pain (TFCC).
From the Blog
- Hand Therapy After Surgery: supervised rehab is essential after TFCC repair.
- Ergonomic Tips for Hand Pain: strategies that reduce ulnar-side wrist load.
Watch: TFCC tear education
Short videos from Dr. Loredo's YouTube and Facebook channels.