Flexor tendon injury is a cut, rupture, or avulsion of one or both flexor tendons that bend the finger. The Verdan classification divides the flexor tendon system into five zones from fingertip to distal forearm; Zone II in the proximal finger is the most technically demanding because both flexor tendons share a narrow fibro-osseous tunnel. Prompt evaluation matters because cut tendons retract and become harder to repair as days pass. Dr. Loredo performs primary repair with multi-strand core sutures, places patients on early controlled motion protocols (Duran passive, Kleinert dynamic, or place-and-hold), and performs tenolysis when adhesions limit gliding after the tendon has healed.
The Anatomy of the Flexor Tendons
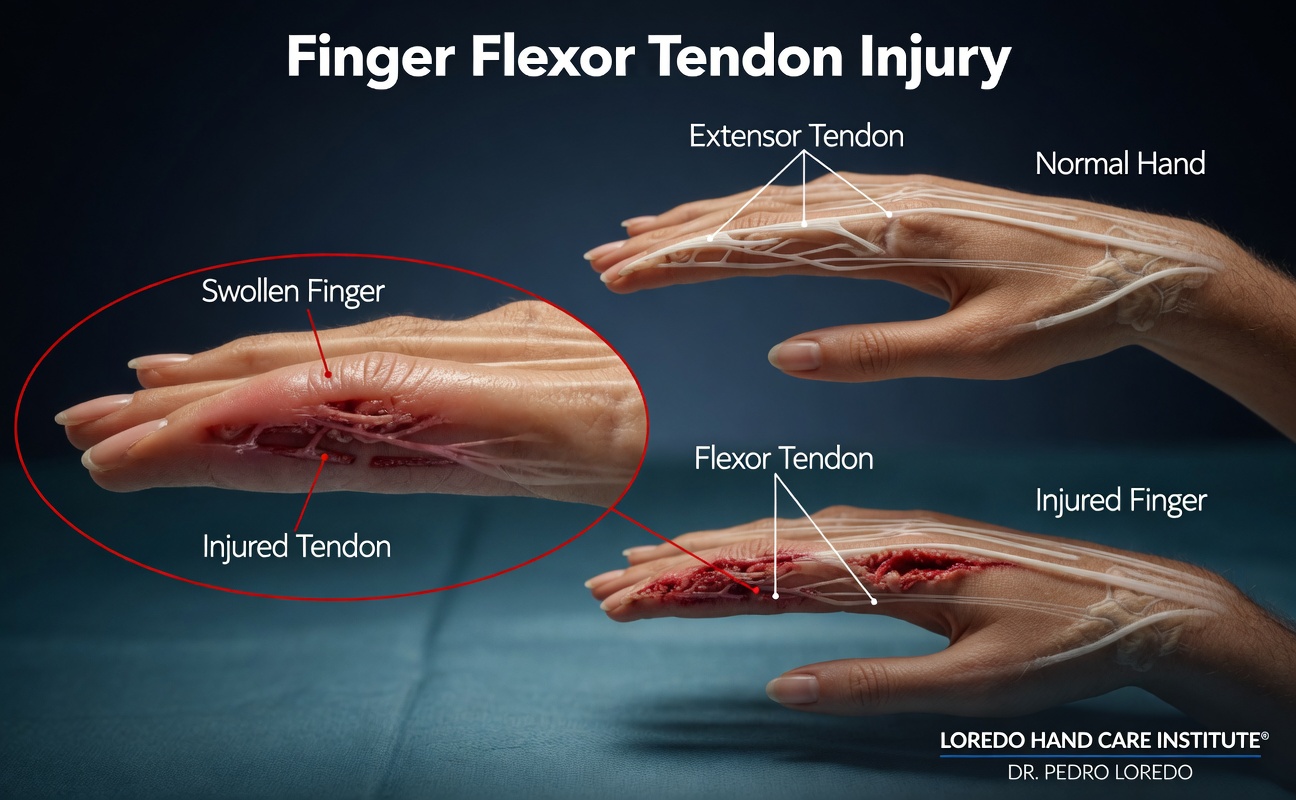
Each finger has two flexor tendons. The flexor digitorum profundus (FDP) bends the fingertip joint and inserts on the distal phalanx. The flexor digitorum superficialis (FDS) bends the middle joint and inserts on the middle phalanx. The thumb has a single flexor tendon, the flexor pollicis longus (FPL), which bends the thumb tip joint. The tendons travel from forearm muscles, through the carpal tunnel, into the palm, and through a series of pulleys (A1 through A5) within the finger.
The flexor tendon sheath surrounds the tendons inside the finger and contains the fluid that lubricates gliding. The pulleys hold the tendons close to the bone during finger flexion, preventing the tendons from bowstringing away. The A2 and A4 pulleys are the most important biomechanically and are preserved during surgery whenever possible.
Verdan divided the flexor tendon system into five anatomic zones to organize injury patterns and treatment. From distal to proximal:
- Zone I: distal to the FDS insertion at the middle phalanx. Only the FDP runs through this zone. Includes jersey finger.
- Zone II: from the A1 pulley at the base of the finger to the FDS insertion. Both FDS and FDP travel through a narrow tunnel together. Called "no man's land" because of the technical difficulty of repair.
- Zone III: the palm, from the distal end of the carpal tunnel to the A1 pulley. The lumbrical muscles arise here.
- Zone IV: within the carpal tunnel.
- Zone V: the distal forearm proximal to the carpal tunnel.
Clinical coding: ICD-10 S66.119A (FPL injury), S66.129A (FDS or FDP injury, finger). SNOMED CT 16996002.
Causes and Risk Factors
- Lacerations from knives, glass, sheet metal, broken bottles, or saws (the most common mechanism)
- Closed avulsion (jersey finger): grabbing a jersey or piece of clothing while the finger is being forcefully extended
- Crush injuries with associated tendon disruption
- Open fractures in which the bone fragment lacerates the tendon
- Workplace injuries involving rotating equipment
- Sports injuries, especially in football, rugby, and martial arts
- Spontaneous rupture, rare but seen in patients with rheumatoid arthritis or after long-standing tendinopathy
Symptoms and Warning Signs

- Inability to bend a specific finger joint (DIP joint for FDP, PIP joint for FDS, IP joint for FPL)
- Visible cut on the palm or finger
- Resting position of the finger more extended than the others (loss of normal cascade)
- Pain, swelling, and bruising along the tendon
- Numbness or tingling in the affected finger from associated digital nerve injury
- Pale or cool fingertip from associated digital artery injury
- In jersey finger, a tender lump in the palm where the avulsed tendon has retracted
How the Diagnosis Is Made
Diagnosis combines a focused history (mechanism, time of injury, hand dominance, occupation) and a careful examination that tests each tendon in isolation.
- FDP test: the examiner holds all the other PIP and DIP joints in extension. The patient bends the fingertip joint of the affected finger. Inability indicates FDP injury.
- FDS test: the examiner holds the other fingers in full extension to neutralize the FDP (which has a common muscle belly). The patient bends the PIP joint of the affected finger. Inability indicates FDS injury.
- FPL test: with the thumb metacarpal stabilized, the patient bends the thumb tip. Inability indicates FPL injury.
- Sensory examination with two-point discrimination on the radial and ulnar sides of each finger to assess the digital nerves.
- Vascular examination: capillary refill at the fingertip and Allen's test to assess the digital arteries.
- X-ray of the affected finger to look for associated bony avulsion (jersey finger may pull off a small fragment of distal phalanx bone) or open fracture.
- Ultrasound or MRI are selectively used in chronic or atypical cases to localize the proximal end of a retracted tendon before surgery.
Treatment Options
Primary Repair (Within 7 to 14 Days)
- Outpatient surgery under regional or local anesthesia
- The wound is extended along proper finger lines for adequate exposure
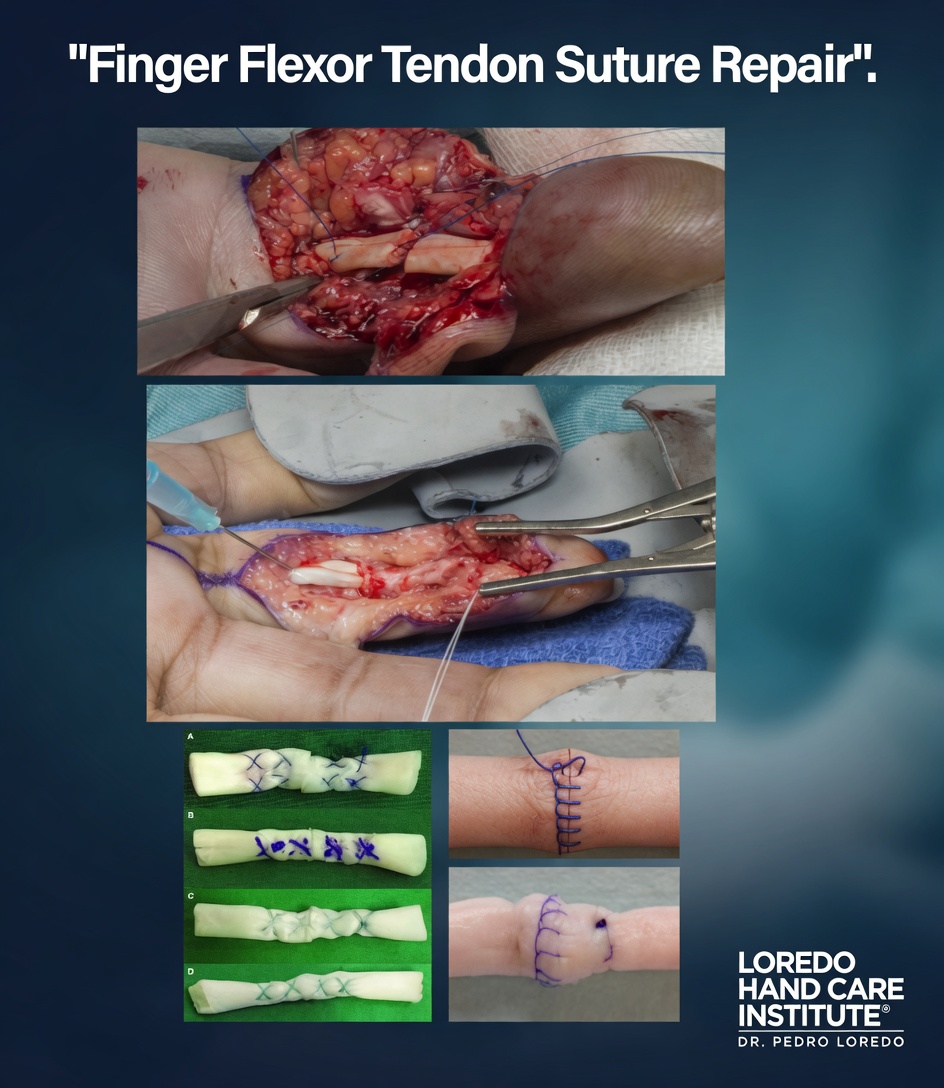
- The proximal end of the tendon is identified and retrieved without injuring the pulley system
- A multi-strand core suture (typically 4 or 6 strands of nonabsorbable suture) plus a circumferential epitendinous suture provides the strength needed for early controlled motion
- The A2 and A4 pulleys are preserved when possible, with venting (partial release) of the A4 only if necessary for tendon glide
- Associated digital nerve and artery injuries are repaired in the same operation under microscope
- The procedure typically takes 60 to 90 minutes for a single tendon
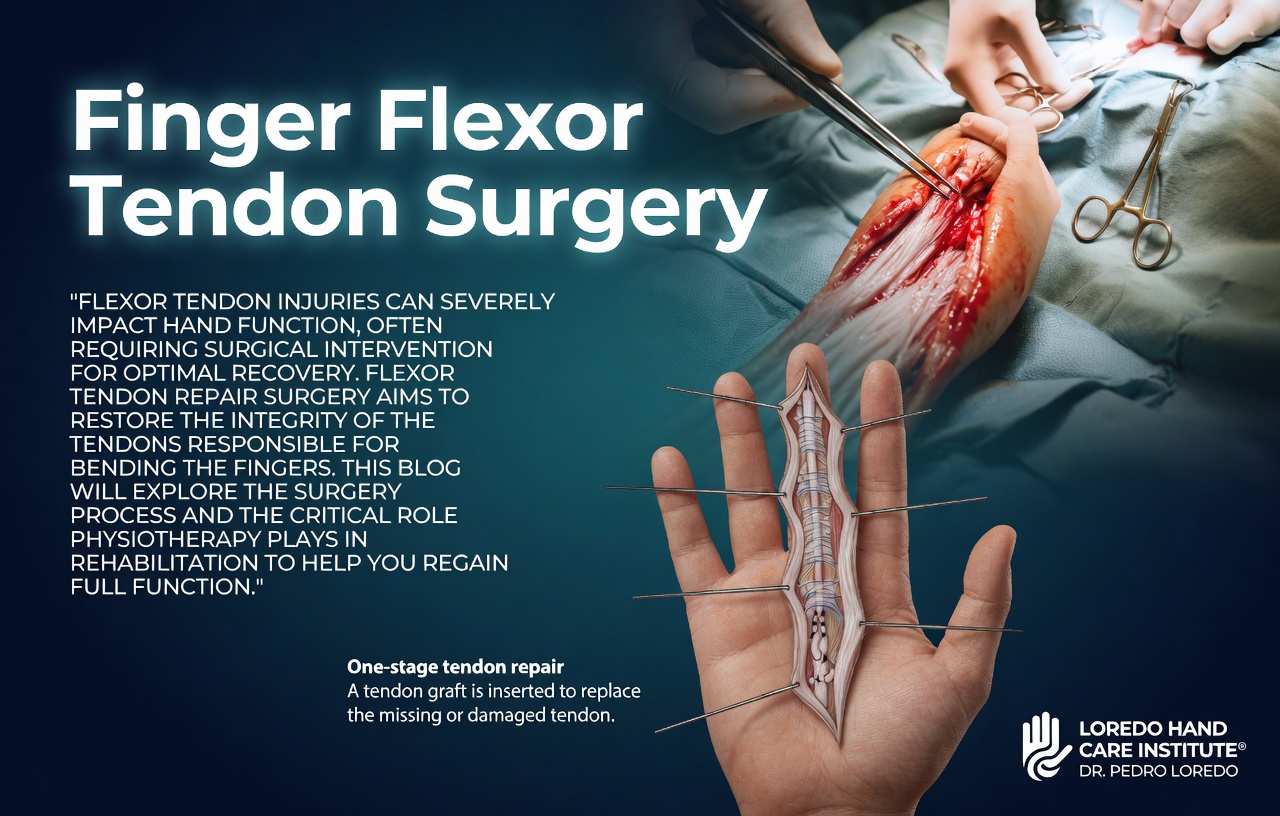
Late Reconstruction
When primary repair is not possible (delayed presentation beyond 3 to 4 weeks, retracted tendon ends, scarred sheath), staged reconstruction is performed. A silicone Hunter rod is placed first to create a smooth gliding tunnel, followed by a free tendon graft (typically the palmaris longus or plantaris) at a second operation 3 to 6 months later.
Tenolysis (For Persistent Stiffness After Healing)
- Performed when adhesions limit gliding after a successful primary repair, usually 3 to 6 months after the original surgery
- Performed under local anesthesia with the patient awake and actively moving the finger
- The surgeon frees the tendon from adhesions and confirms gliding intraoperatively before closing
- Hand therapy starts immediately to prevent re-adhesion
Early Controlled Motion Protocols
Strict immobilization without motion produces poor outcomes. Modern protocols emphasize early protected motion to prevent adhesions while protecting the repair from rupture.
- Duran passive motion: the patient or therapist passively flexes the finger several times per session, multiple sessions per day, for the first 4 to 6 weeks. The repair is not actively loaded.
- Kleinert dynamic traction: rubber band traction holds the finger in slight flexion. The patient actively extends against the rubber band and the band returns the finger to flexion. Provides constant gentle motion.
- Place-and-hold: the therapist passively places the finger in flexion and the patient gently holds the position with light active contraction. Active hold-and-relax progresses over weeks.
Hand therapy is essential to flexor tendon repair recovery and is what separates a good outcome from a stiff finger.
Recovery Timeline
- Day 0: Surgery performed in 60 to 90 minutes for single tendon repair. Custom dorsal blocking splint applied.
- Day 3 to 5: First hand therapy visit. Begin appropriate early controlled motion protocol.
- Week 1 to 4: Daily home program of passive or place-and-hold motion. Splint worn at all times except for therapy.
- Week 4 to 6: Active flexion begins under therapy supervision. Splint progressively decreased.
- Week 6 to 8: Splint discontinued. Active strengthening begins.
- Week 8 to 12: Progressive strengthening. Light gripping returns.
- Month 3 to 6: Return to manual labor and sport. Tendon reaches full strength at 6 months.
Returning to Work and Daily Activity
- Office work: 1 to 2 weeks after repair (in splint, typing with the unaffected hand)
- Light manual labor: 8 to 12 weeks
- Heavy manual labor and contact sport: 4 to 6 months
- Driving: 4 to 6 weeks once out of dorsal blocking splint
Frequently Asked Questions
Why does a finger laceration sometimes need surgery within days?
A cut tendon retracts. The two ends pull apart and become harder to identify and reattach as days pass. Within 7 to 14 days the proximal tendon end shortens and the tendon sheath begins to scar. Beyond 3 to 4 weeks, primary repair often becomes difficult or impossible and reconstructive grafting may be required, which has a longer recovery and somewhat lower success. Prompt evaluation and repair within the first 1 to 2 weeks gives the best functional outcome.
What is Zone II and why is it called no man's land?
Zone II runs from the A1 pulley at the base of the finger to the insertion of the FDS tendon at the middle phalanx. In this zone, both flexor tendons (FDS and FDP) and the digital nerves and arteries pass through a narrow fibro-osseous tunnel. Surgical repair is technically demanding because the two tendons must glide smoothly through the same narrow tunnel after repair. Adhesions are common, and historically results were so poor that the area was called no man's land. Modern multi-strand suture techniques and early controlled motion protocols have substantially improved outcomes, but Zone II remains the most challenging zone for flexor tendon repair.
What is jersey finger?
Jersey finger is a closed avulsion of the FDP tendon from its attachment on the distal phalanx, classically caused by grabbing a jersey or piece of clothing while the finger is being forcefully extended. The patient cannot bend the fingertip joint of the affected finger. Jersey finger is a Zone I injury and requires prompt surgical reattachment, ideally within 7 to 10 days, because the avulsed tendon retracts into the palm and loses its blood supply quickly. Late presentations may require staged tendon grafting.
Can I move my finger after tendon repair?
Yes, in a controlled way. Modern protocols emphasize early protected motion to prevent adhesions and improve gliding. The Duran passive motion, Kleinert dynamic traction, and place-and-hold protocols all begin within the first week of surgery and progress over 6 to 12 weeks under hand therapy supervision. Strict immobilization without motion produces worse outcomes and is no longer the standard of care for most flexor repairs. Hand therapy is essential and is what separates a good repair from a stiff finger.
What if my finger stays stiff after the tendon heals?
Adhesions between the repaired tendon and the surrounding sheath are the most common reason for persistent stiffness. When stiffness has not improved after 3 to 6 months of consistent hand therapy following a successful primary repair, tenolysis (a second operation that frees the tendon from adhesions) is considered. Tenolysis is performed under local anesthesia with the patient awake and actively moving the finger so the surgeon can confirm that gliding has been restored before closing.
When to Call the Doctor
Call our office or go to an emergency department promptly if you experience any of the following:
- A cut on the palm, thumb, or finger that does not allow you to bend a specific joint
- A finger that cannot bend the fingertip joint (suggests FDP or jersey finger)
- A finger that cannot bend the middle joint while the others are held in extension (suggests FDS injury)
- Numbness in part of a finger after a laceration (associated nerve injury)
- Pale, cool, or non-bleeding fingertip after an injury (vascular injury, requires emergency care)
- A grabbing or pulling injury followed by pain and inability to bend the fingertip (suspect jersey finger)
After surgery, call promptly if you experience fever over 101°F, expanding redness or drainage at the incision, severe pain not controlled by medication, splint that becomes too tight, or any sense that the tendon has snapped (sudden loss of motion that you previously had).
Open lacerations with active bleeding, pulseless cold fingertips, or amputation injuries are emergencies. Call 911 or go to the nearest emergency department immediately.
Related Conditions
- Extensor Tendon Injury: the dorsal counterpart with its own zone classification (I-VIII). Often coexists in crush or laceration injuries that involve both surfaces of the hand.
- Trigger Finger: a different flexor tendon problem caused by stenosing tenosynovitis at the A1 pulley. Not traumatic, but in the same anatomic zone.
- Hand and Finger Fractures: open fractures often have associated tendon injuries that must be addressed in the same operation.
- Carpal Tunnel Syndrome: tendon injuries at Zone IV (within the carpal tunnel) require a release of the transverse carpal ligament and can produce postoperative carpal tunnel symptoms.
- Dupuytren's Contracture: dense palmar scar from late Dupuytren's can occasionally be confused with chronic Zone III tendon injury on physical examination.
From the Blog
- Mallet Finger and Jersey Finger: When to Worry: jersey finger is the most time-sensitive flexor avulsion.
- Hand Therapy After Surgery: Duran/Kleinert/Indiana protocols and the role of a Certified Hand Therapist.
Watch: Flexor tendon injury education
Short videos from Dr. Loredo's Instagram and Facebook channels.