Extensor tendon injuries affect the tendons that straighten the fingers and thumb. The modified Verdan classification organizes these tendons into eight zones from the fingertip to the distal forearm, and treatment depends on the zone and whether the injury is open or closed. Two specific named injuries dominate the field: mallet finger (Zone I, terminal extensor disruption at the DIP joint, treated with continuous DIP extension splinting for 8 weeks) and boutonniere deformity (Zone III, central slip rupture at the PIP joint, treated with PIP extension splinting if caught early). Open lacerations require primary surgical repair. Outcomes are generally better than for flexor tendon injuries because of simpler anatomy and lower adhesion rates.
The Anatomy of the Extensor Mechanism
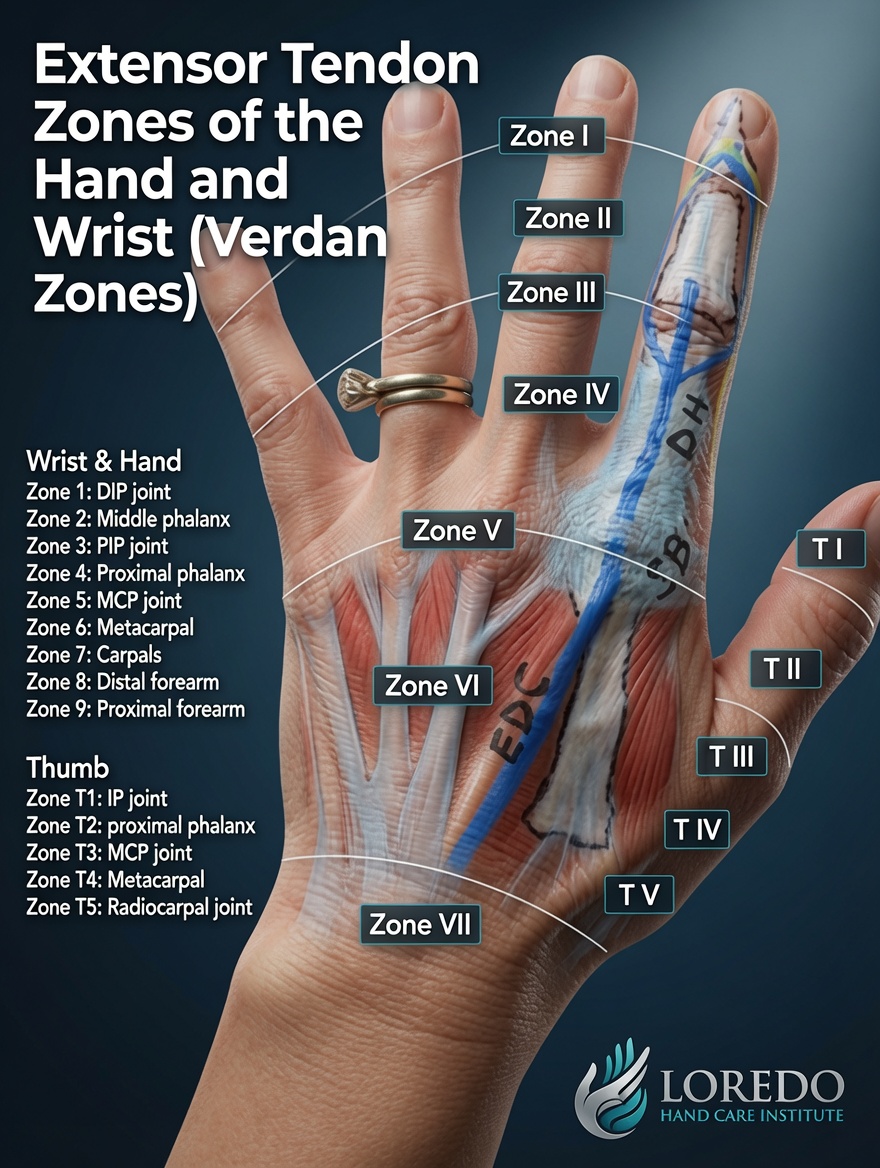
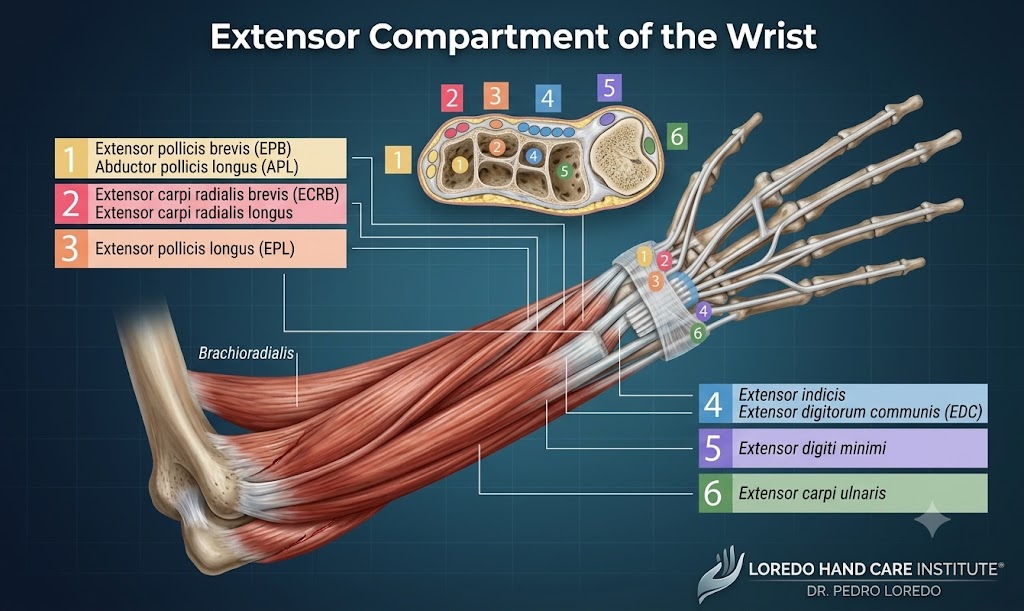
The extensor mechanism is a flat, ribbon-like structure that runs over the back of each finger from the dorsum of the hand to the fingertip. At the DIP joint it terminates as the terminal extensor tendon. At the PIP joint it splits into a central slip (which inserts on the middle phalanx) and two lateral bands (which run on either side of the joint and rejoin distally). Over the proximal phalanx and MCP joint, the extensor digitorum communis tendon is connected to its neighbors by juncturae tendinum, fibrous bands that explain why one finger can sometimes still extend even when its tendon is cut. At the wrist, six dorsal extensor compartments hold the wrist and finger extensor tendons in place under the extensor retinaculum.
The modified Verdan classification organizes these tendons into eight anatomic zones. The odd-numbered zones lie over the joints (I, III, V, VII), and the even-numbered zones lie over the bones between the joints (II, IV, VI, VIII). The system was designed so that the joint-level zones, which are the most challenging to repair, all share the same odd numbering scheme.
Clinical coding: ICD-10 S66.30 (unspecified injury of extensor muscle, fascia, and tendon, finger). SNOMED CT 16996003.

Causes and Risk Factors
- Jamming injuries: a ball or other object strikes the extended fingertip and forces it into flexion (the classic mallet finger mechanism)
- Lacerations from knives, glass, sheet metal, or saws on the back of the hand or finger
- Fight bite injuries: a bite over the MCP joint that lacerates Zone V tendons (a true emergency due to high infection risk)
- Closed forced flexion of the PIP joint against an extended finger, producing central slip rupture (boutonniere)
- Crush injuries with associated tendon disruption
- Spontaneous rupture in patients with rheumatoid arthritis, particularly the EPL tendon at Lister's tubercle
- Open fractures with associated tendon injury
Symptoms and Warning Signs
- Inability to fully straighten a specific finger joint
- Drooping fingertip (the classic mallet finger appearance)
- Inability to straighten the middle joint (suggests Zone III central slip injury)
- Visible cut on the back of the hand or finger
- Pain over a specific joint or tendon segment
- Swelling and bruising along the dorsal aspect
- Boutonniere deformity that develops 2 to 4 weeks after a missed Zone III injury (the lateral bands shift and the appearance worsens over weeks)
- Inability to extend the thumb at the IP joint (suggests EPL rupture, common in rheumatoid disease and after a healed distal radius fracture)
How the Diagnosis Is Made
The evaluation begins with the mechanism of injury (jam, cut, fight bite, fall) and a careful examination of every joint of every finger.
- Inspection of resting cascade: a finger that fails to maintain the normal cascade with its neighbors suggests an extensor tendon imbalance.
- Active extension test for each joint: the patient extends each joint individually against gravity and against light resistance. Inability points to the level of injury.
- Elson's test for central slip integrity: the patient flexes the PIP joint over the edge of a table and tries to extend it. With central slip rupture, the DIP joint becomes rigid and the PIP cannot extend.
- Boyes' test for chronic boutonniere: the inability to flex the DIP joint with the PIP held in extension confirms a chronic boutonniere deformity.
- X-ray of the affected finger is obtained for all closed mallet injuries to identify a bony fragment, and for any laceration to look for retained foreign body or open fracture.
Specific Injuries and Their Treatment
Mallet Finger (Zone I)
Avulsion or rupture of the terminal extensor tendon at the DIP joint. The patient cannot straighten the fingertip. Treatment of closed mallet injuries is continuous DIP extension splinting for 8 weeks. The PIP joint is left free. Any flexion of the DIP during the 8-week period restarts the clock. After 8 weeks, the splint is worn at night for an additional 2 to 4 weeks while the patient gradually resumes flexion. Open mallet injuries or those with a large displaced bony fragment may require surgical pinning or repair.

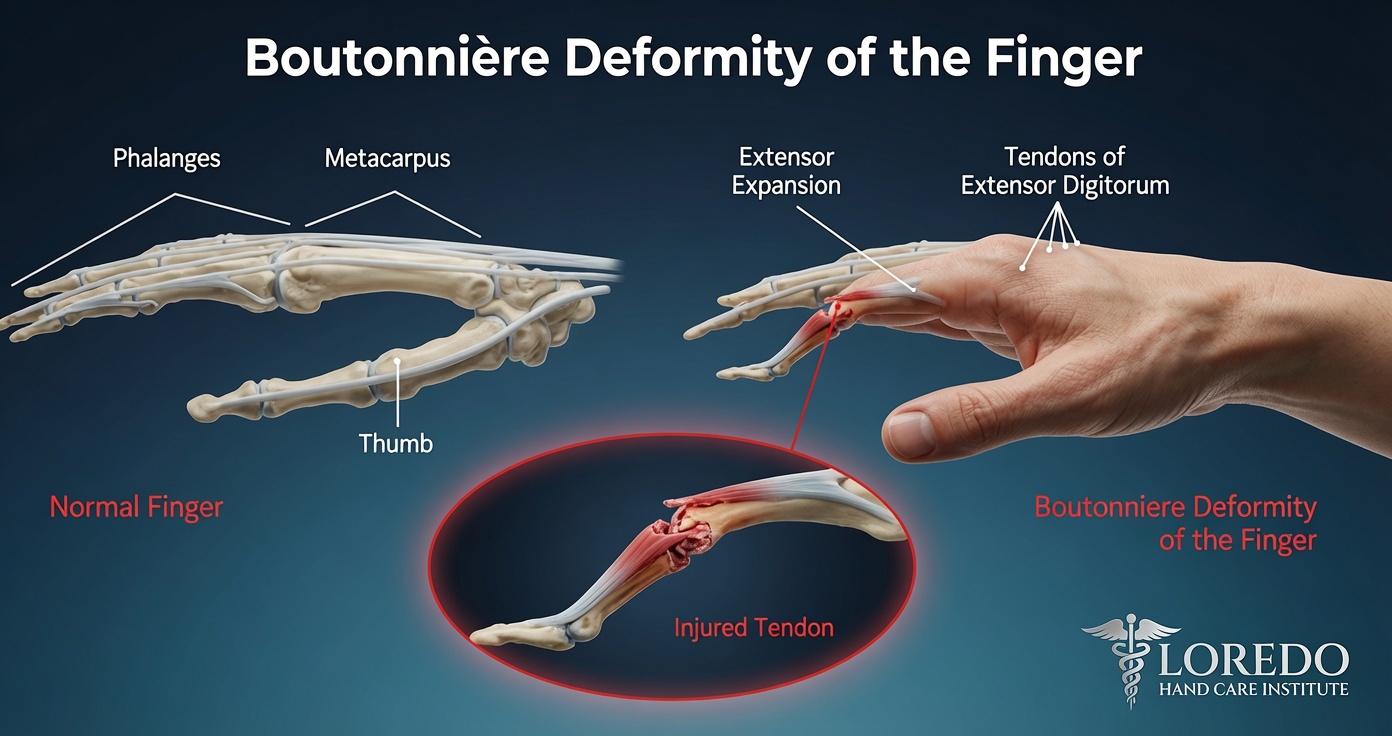
Boutonniere Deformity (Zone III)
Disruption of the central slip at the PIP joint. Acute closed injuries are treated with PIP extension splinting for 6 weeks while the DIP and MCP joints remain free to move. Open lacerations are repaired primarily. Chronic boutonniere (more than 4 to 6 weeks old) is harder to treat. Reconstruction options include central slip reconstruction with local tissue, lateral band relocation, or staged reconstruction. Outcomes are more guarded than for acute injury.
Zone V Lacerations (MCP Joint Level)
Particularly important because of the fight bite mechanism. A laceration over the MCP joint after a punch is highly suspicious for a tooth penetration into the joint. These wounds require surgical exploration, copious irrigation, primary tendon repair when possible, and antibiotic coverage. Untreated fight bites lead to septic arthritis and devastating long-term joint damage.
Zones VI through VIII Lacerations
Open lacerations on the dorsum of the hand, dorsal wrist, or distal forearm are repaired primarily with multi-strand sutures. Outcomes are generally good with appropriate hand therapy.
Treatment Options for Open Lacerations
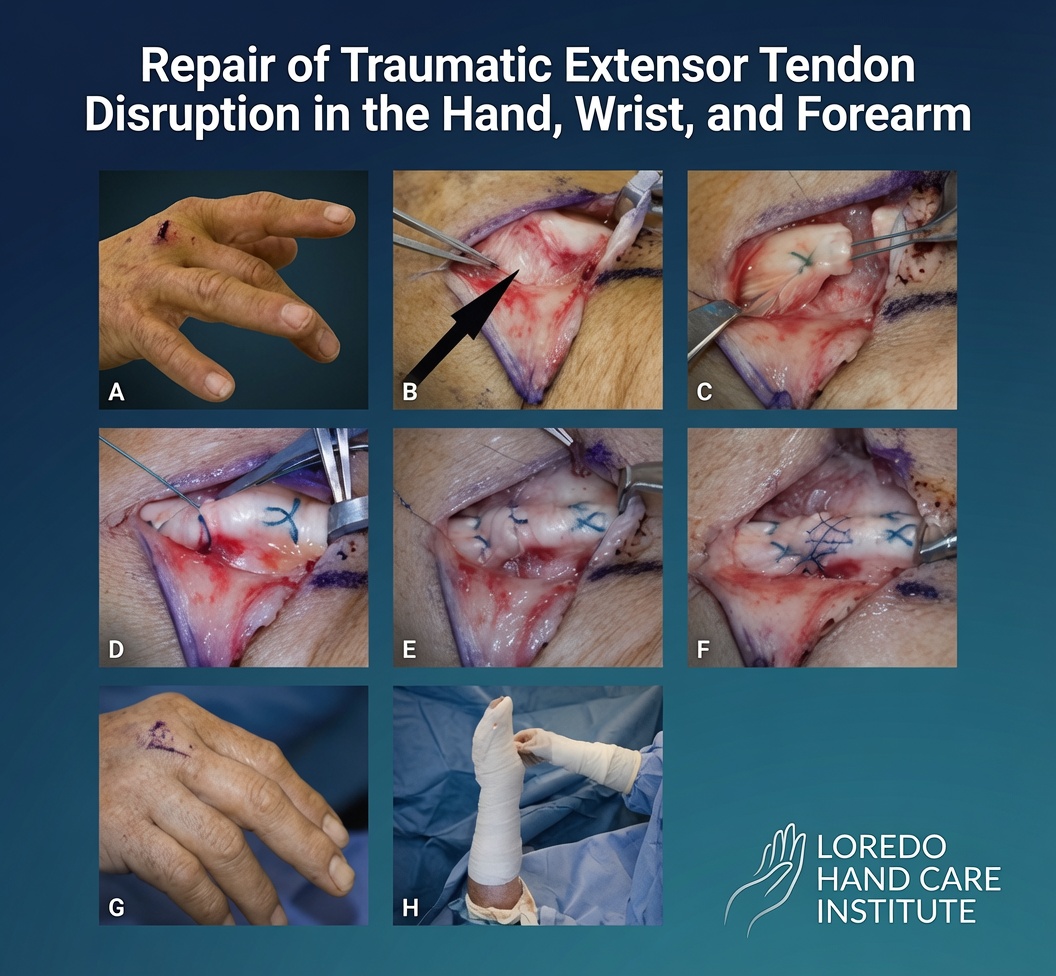
- Primary surgical repair with multi-strand core sutures plus an epitendinous suture for tendon ends that can be approximated
- Wound irrigation and antibiotic coverage for any open injury, especially fight bites
- Bony reattachment with suture anchor or pin fixation when there is an associated avulsion fragment
- Tendon graft for delayed presentations where the proximal end has retracted and primary repair is not possible
- Relative motion splinting protocols for early controlled motion after Zone IV through Zone VII repairs
Recovery Timeline

- Closed mallet finger (Zone I): 8 weeks of continuous DIP extension splinting plus 2 to 4 weeks of nighttime splinting. Full activity at 10 to 12 weeks.
- Acute closed boutonniere (Zone III): 6 weeks of continuous PIP extension splinting, then progressive flexion under therapy supervision. Full activity at 10 to 12 weeks.
- Open repairs in Zones IV-VII: custom relative motion splint for 4 to 6 weeks, progressive active motion under therapy. Full activity at 8 to 12 weeks.
- Open Zone V (fight bite): antibiotics, surgical irrigation, primary repair if clean. Recovery as for other Zone V injuries with very close follow-up.
- Chronic boutonniere reconstruction: 8 to 12 weeks of structured therapy. Outcomes are more guarded.
Returning to Work and Daily Activity
- Office work in a finger or hand splint: within days to a week
- Light manual labor: 4 to 6 weeks for closed mallet/boutonniere; 6 to 8 weeks after primary repair
- Heavy manual labor and contact sport: 10 to 12 weeks
- Driving: 1 to 2 weeks once splint allows safe vehicle control
Frequently Asked Questions
What is mallet finger?
Mallet finger is a Zone I extensor tendon injury at the DIP joint. The terminal extensor tendon either tears or is avulsed with a small fragment of the distal phalanx, and the patient cannot fully straighten the fingertip. Closed mallet injuries are treated with continuous DIP extension splinting for 8 weeks (no flexion allowed during this period). Open mallet injuries or those with a large bony fragment may need surgical repair. Outcomes are excellent when splinting is consistent.
What is boutonniere deformity?
Boutonniere deformity is a flexion contracture of the PIP joint with hyperextension of the DIP joint, resulting from a Zone III injury to the central slip of the extensor mechanism over the back of the middle joint. Acutely, after a jamming injury or laceration over the PIP joint, the patient cannot fully straighten the middle joint. Without prompt treatment over 2 to 4 weeks, the lateral bands shift below the PIP joint axis and the deformity becomes fixed. Closed acute injuries are treated with PIP extension splinting for 6 weeks. Chronic boutonniere requires surgical reconstruction and has more guarded results.
How is extensor tendon repair different from flexor repair?
Extensor tendons are anatomically different. They are flatter and thinner than flexor tendons and lie just under the skin without a tight tunnel system. Surgical repair is more straightforward, complications are fewer, and outcomes are generally better. Stiffness is still a concern, particularly in Zone III and Zone V (over the knuckle), but adhesions are less limiting than they are after flexor repair. Hand therapy with relative motion splinting protocols has further improved outcomes.
Do all extensor injuries need surgery?
No. Closed Zone I injuries (mallet finger) and many closed Zone III injuries (acute boutonniere) heal well with splinting alone when caught early and treated consistently. Open lacerations always require surgical repair. Chronic boutonniere, lacerations with retracted tendon ends, and injuries with associated bone or joint involvement also need surgery. The decision is made on a case-by-case basis after a careful examination and X-ray.
How long must I wear a mallet finger splint?
A mallet finger splint must be worn continuously for 8 weeks, including during showers (the splint is removed only briefly for skin care while the finger is held in extension by another finger or against a flat surface). Any flexion of the DIP joint during the 8 weeks restarts the clock. After the 8-week period, the splint is worn at night for an additional 2 to 4 weeks while the patient gradually resumes finger flexion. Patient compliance with the splinting protocol is the single most important factor in achieving a good outcome.
When to Call the Doctor
Call our office promptly if you experience:
- A drooping fingertip after a jamming injury (suspect mallet finger)
- Inability to straighten the middle joint of a finger after a jam or cut (suspect boutonniere)
- A cut on the back of the hand or finger that affects motion
- A laceration over the knuckle after a punch (treat as a fight bite emergency until proven otherwise)
- Sudden inability to extend the thumb tip in a patient with rheumatoid arthritis or after a healed wrist fracture (suspect EPL rupture)
- A finger that develops a worsening deformity over 1 to 4 weeks after a seemingly minor injury
After surgery or splinting, call promptly if you experience fever, expanding redness, drainage at the incision, severe pain not controlled by medication, or a splint that becomes loose or wet.
Open lacerations with active bleeding, fight bites over the knuckle, or amputation injuries are emergencies. Call 911 or go to the nearest emergency department immediately.
Related Conditions
- Flexor Tendon Injury: the volar counterpart with its own zone classification (I-V). Can coexist with extensor injuries in crush trauma involving both surfaces of the hand.
- Hand and Finger Fractures: distal phalanx fractures often accompany mallet finger injuries when a bony fragment is avulsed. Open hand fractures often have associated tendon injury.
- Hand and Wrist Arthritis: spontaneous extensor tendon rupture, particularly the EPL or extensor digitorum communis tendons, is a recognized complication of rheumatoid arthritis.
- Trigger Finger: a different tendon problem on the volar side, listed because patients sometimes have multiple tendon issues at once.
- Wrist Tendonitis: inflammation in any of the six dorsal extensor compartments. The compartmental anatomy is the same anatomy as the dorsal extensor zones.
From the Blog
- Mallet Finger and Jersey Finger: When to Worry: fingertip tendon avulsions with very different urgency.
- Hand Therapy After Surgery: supervised tendon-glide protocols matter most for tendon repairs.
Watch: Extensor tendon injury education
Short videos from Dr. Loredo's Instagram and Facebook channels.