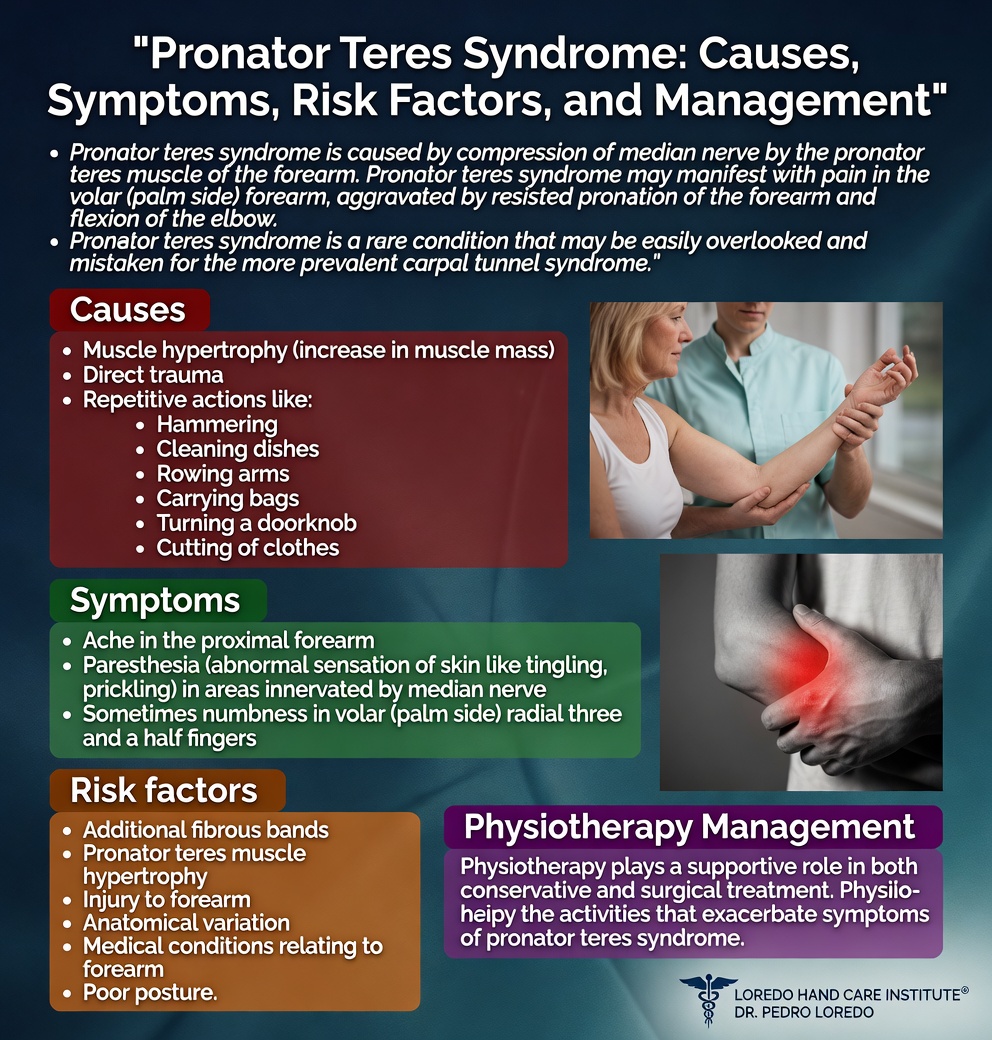
Pronator teres syndrome is compression of the median nerve in the proximal forearm at one or more of four potential anatomic narrow points. Patients present with aching pain in the volar forearm and median-distribution numbness in the thumb, index, middle, and half of the ring finger. Unlike carpal tunnel syndrome, the symptoms are not nocturnal and are reproduced by repetitive forearm rotation rather than by wrist position. Treatment ranges from activity modification and splinting to surgical decompression of all four compression sites: the lacertus fibrosus, both heads of the pronator teres, and the proximal FDS arch.
The Anatomy of the Proximal Forearm
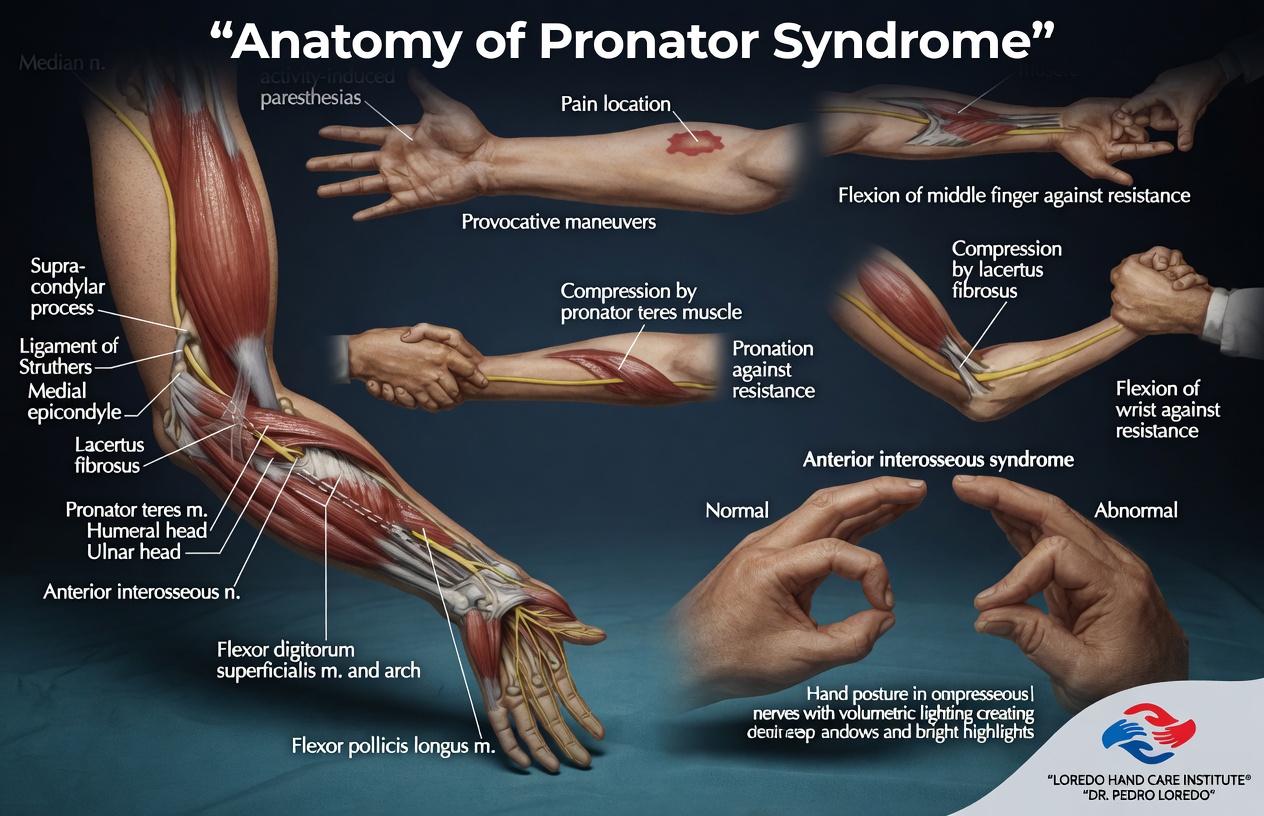
The median nerve enters the forearm at the elbow and immediately encounters several potential compression points before it reaches the carpal tunnel at the wrist. From proximal to distal these are: the ligament of Struthers (a fibrous band found in approximately 1 percent of patients above the medial epicondyle), the lacertus fibrosus (a thick fibrous extension of the biceps tendon at the elbow), the space between the two heads of the pronator teres muscle (the humeral head and the ulnar head), and the proximal arch of the flexor digitorum superficialis muscle.
In pronator teres syndrome, one or more of these structures compresses the median nerve in a dynamic pattern. Repetitive forearm rotation, particularly forced pronation against resistance, is the most common trigger. The condition is named for the pronator teres because that is the most common single compression point, but successful surgical treatment requires releasing all four potential compression sites because partial release is associated with persistent or recurrent symptoms.
Pronator teres syndrome is sometimes confused with anterior interosseous nerve (AIN) syndrome. The two affect different median nerve fibers in similar locations. Pronator teres syndrome compresses the main median nerve and produces both pain and sensory symptoms. AIN syndrome affects only the deep motor branch and produces a characteristic motor pattern (inability to make the OK sign) without pain or numbness.
Clinical coding: ICD-10 G56.11 (lesion of median nerve, upper limb, other). SNOMED CT 73927008.
Causes and Risk Factors
- Repetitive forearm pronation, particularly under load
- Manual occupations: mechanics, butchers, electricians, plumbers, carpenters
- Weight training with heavy gripping and pronation, particularly biceps curls and rows
- Forceful gripping with the elbow extended
- Hypertrophy of the pronator teres muscle in heavy manual workers
- Trauma or fracture in the proximal forearm
- Anatomic variants: a tendinous (rather than muscular) Arcade of Struthers or fibrous bands within the pronator
- Diabetes, which makes nerves more vulnerable to compression at any site
Symptoms and Warning Signs
- Aching pain in the volar (front) forearm, often worse with use
- Numbness or tingling in the thumb, index, middle, and the radial half of the ring finger
- Symptoms that worsen with manual work, gripping, and forearm rotation
- Symptoms that do not wake the patient at night (a key contrast with carpal tunnel)
- Tenderness over the pronator teres muscle in the proximal volar forearm
- Mild thumb or index weakness in some cases, but usually no measurable motor loss
- Pain that may radiate up to the elbow or down to the wrist
- Symptoms reproduced by specific provocative tests rather than by wrist position
How the Diagnosis Is Made
Pronator teres syndrome is a clinical diagnosis. Dr. Loredo performs three standard provocative tests to localize the compression:
- Resisted pronation with elbow extended: the patient pronates the forearm against the examiner's resistance with the elbow held in full extension. Reproduction of forearm pain and tingling in median-distribution fingers is positive.
- Resisted long-finger flexion (FDS arch test): the patient flexes the middle finger against resistance at the PIP joint with the wrist neutral. Reproduction of pain implicates the proximal arch of the FDS as a compression site.
- Tinel's sign over the pronator teres: tapping over the pronator muscle in the proximal volar forearm reproduces tingling in the median nerve distribution.
- Resisted elbow flexion at 120 degrees with supination: reproduces symptoms when the lacertus fibrosus is the compression site.
Confirmatory testing includes electrodiagnostic studies (EMG and nerve conduction studies) that may show median nerve slowing across the proximal forearm. Studies are often normal because the compression is dynamic. A normal study does not rule out the diagnosis when the clinical picture is consistent. MRI of the proximal forearm is selectively used to look for muscle hypertrophy, an accessory band, or a space-occupying lesion. A diagnostic injection of local anesthetic into the area between the pronator heads can be useful in difficult cases.
Non-Surgical Treatment Options
At least 3 to 6 months of structured conservative care is appropriate before considering surgery.
- Activity modification: reduce or rotate the repetitive forearm pronation that produces symptoms.
- Forearm splinting with the forearm in mid-rotation, particularly at night.
- Targeted hand therapy with median nerve glide exercises, gentle stretching, and pronator strengthening once acute symptoms settle.
- Topical and oral nonsteroidal anti-inflammatory medication.
- Selective corticosteroid injection into the pronator teres or under the lacertus fibrosus under ultrasound guidance.
- Workplace ergonomic assessment to identify and modify aggravating tasks.
Surgical Options
Surgery is considered when symptoms persist beyond 3 to 6 months of structured conservative care and when the patient is significantly limited in work or daily activity.
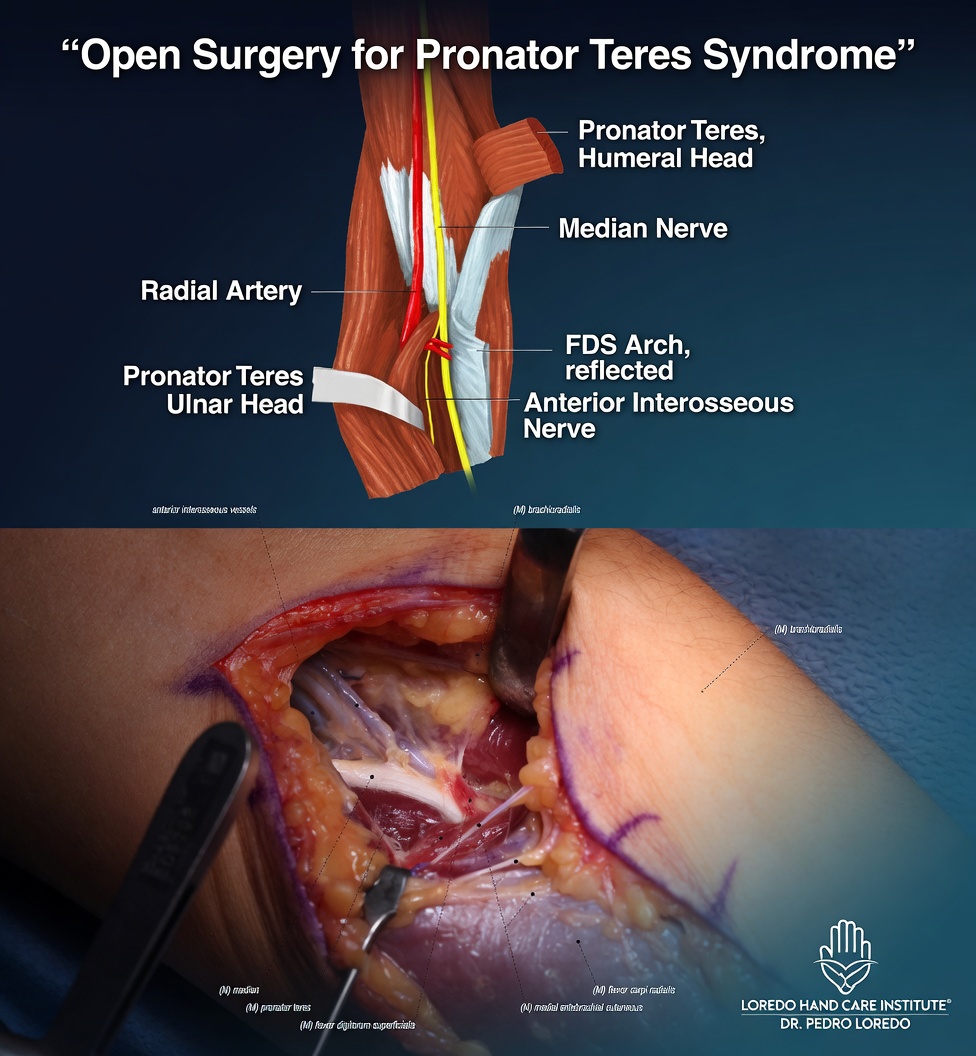
Median Nerve Decompression in the Proximal Forearm
- Curvilinear incision in the volar proximal forearm
- Identification of the median nerve at the elbow and tracing distally
- Release of the lacertus fibrosus
- Division of any tight fibers between the humeral and ulnar heads of the pronator teres
- Release of the proximal FDS arch
- Release of the ligament of Struthers if present
- Procedure takes 45 to 60 minutes under regional anesthesia
- Soft dressing and removable splint for the first week
Combined Procedure with Carpal Tunnel Release
Some patients with severe median nerve symptoms have both pronator teres syndrome and carpal tunnel syndrome, called the double crush phenomenon. Both compression points can be addressed in the same operation through separate small incisions when the diagnosis is established.
Surgical success rates for pronator teres syndrome decompression are 70 to 85 percent across published series. Patient selection and the precision of preoperative diagnosis are the most important variables.
Recovery Timeline
- Day 0: Procedure performed in 45 to 60 minutes under regional anesthesia. Removable splint applied.
- Day 1 to 7: Light hand and finger motion several times per day. Bandage care per instructions.
- Week 1 to 2: First follow-up. Sutures removed. Begin gentle elbow and forearm range of motion.
- Week 2 to 6: Progressive forearm range of motion and gentle strengthening. Hand therapy with nerve gliding exercises.
- Week 6 to 12: Sensory recovery progressing. Return to manual labor and athletic activity in this window.
- Month 3 to 6: Final results assessed. Severe long-standing cases may continue to improve gradually beyond 6 months.
Returning to Work and Daily Activity
- Office or desk work: 1 to 2 weeks after surgery
- Light manual labor: 4 to 6 weeks
- Heavy manual labor: 8 to 12 weeks with attention to the technique that produced symptoms
- Weight training: 6 to 8 weeks for upper body, with progressive return through coached technique
- Driving: 1 to 2 weeks once off pain medication and able to grip the wheel comfortably
Frequently Asked Questions
How is pronator teres syndrome different from carpal tunnel?
Both conditions affect the median nerve and produce numbness in the same fingers. The differences are in location of pain, the absence of night symptoms in pronator teres syndrome, and the response to provocative tests. Carpal tunnel pain is at the wrist and classically wakes patients at night. Pronator teres syndrome produces aching pain in the volar forearm that is worse with manual work and not nocturnal. Resisted pronation, resisted long-finger flexion, and tenderness over the pronator muscle reproduce pronator teres pain but not carpal tunnel pain. Some patients have both conditions, called the double crush phenomenon.
Why are there four potential compression sites?
The median nerve passes through several anatomic narrow points in the proximal forearm. From proximal to distal: the ligament of Struthers (when present), the bicipital aponeurosis (lacertus fibrosus) at the elbow, between the two heads of the pronator teres, and beneath the proximal arch of the flexor digitorum superficialis. Each is a potential compression point. Surgery must release all four because partial release leads to recurrent or persistent symptoms.
Is pronator teres syndrome the same as anterior interosseous nerve syndrome?
No. They both involve median nerve branches in the forearm, but they affect different fibers and present differently. Pronator teres syndrome compresses the main median nerve and produces forearm pain plus sensory symptoms in the median distribution. Anterior interosseous nerve (AIN) syndrome affects only the deep motor branch and produces weakness of the flexor pollicis longus, the flexor digitorum profundus to the index finger, and the pronator quadratus, with a characteristic inability to make the OK sign. AIN syndrome is painless and motor-only. Pronator teres syndrome is painful and has sensory features.
How long is conservative treatment before surgery?
At least 3 to 6 months of activity modification, splinting, hand therapy, and selective NSAID use is appropriate before considering surgery. Many cases improve with simple changes in repetitive forearm rotation patterns. Surgery is reserved for patients who have completed structured conservative care and continue to be limited in work or daily activity.
What does median nerve decompression in the forearm involve?
The procedure is performed through an incision in the volar forearm. The median nerve is identified and traced from the elbow down through all four potential compression sites. Each tight structure is divided to free the nerve. The procedure takes 45 to 60 minutes under regional anesthesia. Soft dressing and a removable splint are used for the first week. Recovery is similar to other peripheral nerve decompressions, with sensory improvement typically progressing over 6 to 12 weeks.
When to Call the Doctor
Before treatment, call our office for evaluation if you experience:
- Forearm aching pain plus numbness or tingling in the thumb, index, or middle finger
- Symptoms that worsen with manual work or forearm rotation but do not wake you at night
- Persistent symptoms after appropriate carpal tunnel evaluation has been negative or treatment has failed
- Failure to improve with structured conservative care
After surgery, call promptly if you experience fever over 101°F, expanding redness or drainage at the incision, severe pain not controlled by medication, or new numbness or weakness in the hand.
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Carpal Tunnel Syndrome: median nerve compression at the wrist. The most important alternative diagnosis. Differentiated by the presence of nocturnal symptoms in carpal tunnel and forearm pain in pronator teres syndrome. The two can coexist (double crush).
- Cubital Tunnel Syndrome: ulnar nerve compression at the elbow. Affects different fingers (ring and small) and a different nerve.
- Radial Tunnel Syndrome: PIN compression on the lateral side of the forearm. The lateral counterpart to pronator teres syndrome on similar repetitive rotation patterns.
- Guyon's Canal Syndrome: ulnar nerve compression at the wrist. Listed because patients with persistent forearm or hand symptoms sometimes have multiple coexisting nerve issues.
- Hand and Wrist Arthritis: arthritis can refer pain into the forearm and rarely produce confusion with nerve compression diagnoses.
From the Blog
- The Median Nerve Explained: full anatomy and the four main compression sites.
- Early Signs of Carpal Tunnel: differential diagnosis with the more common compression site.
Watch: Pronator teres syndrome education
Short videos from Dr. Loredo's YouTube and Facebook channels.