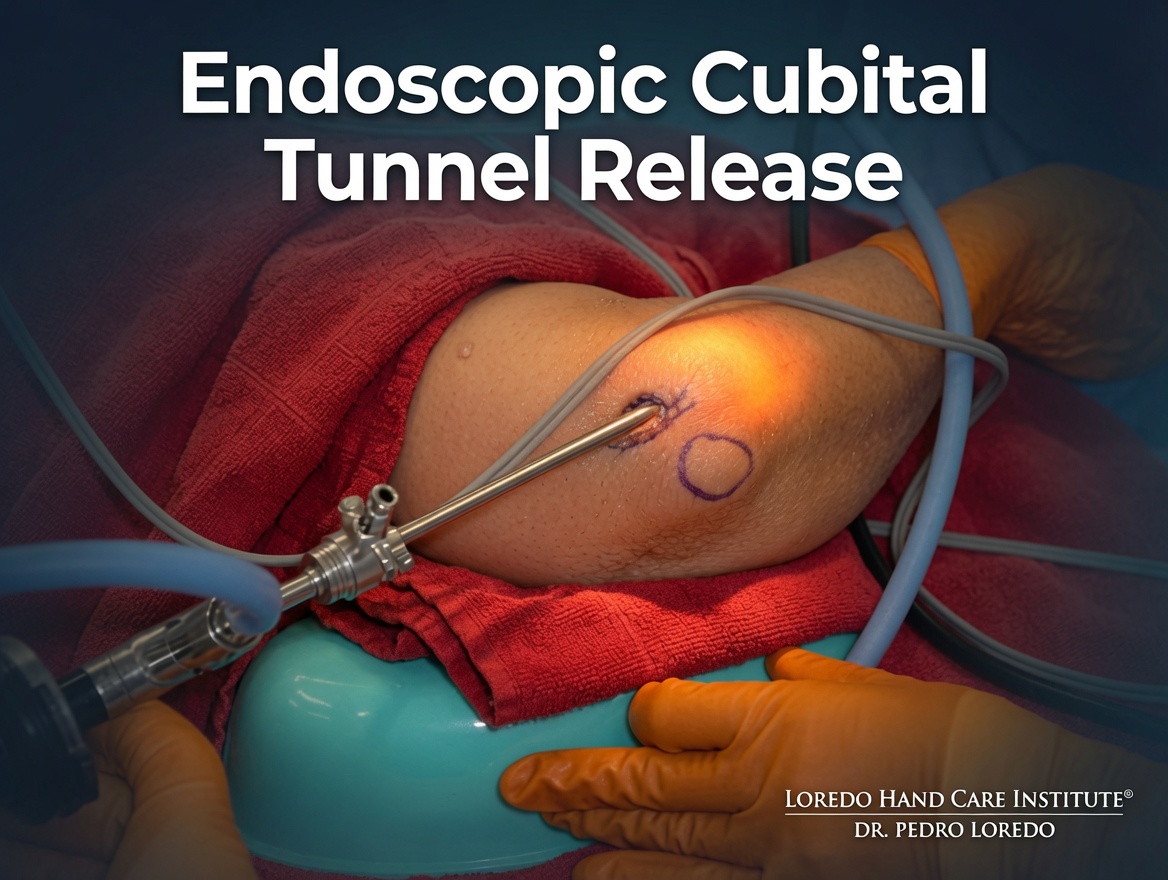
Endoscopic cubital tunnel release is a minimally invasive procedure to decompress the ulnar nerve at the elbow. Through a single 2 cm posteromedial incision, Dr. Loredo introduces a specialized endoscope to visualize the ulnar nerve along its full length and release the structures that compress it: the medial intermuscular septum proximally, Osborne's ligament at the cubital tunnel, the leading edge of the FCU muscle, and the deep fascia distally. The procedure takes 30 to 60 minutes under MAC anesthesia with local block. Most patients return to office work in 1 to 2 weeks and manual labor in 4 to 6 weeks. Compared to open transposition, the endoscopic approach has less postoperative pain, a smaller scar, and a faster return to function.
What Is Endoscopic Cubital Tunnel Release?
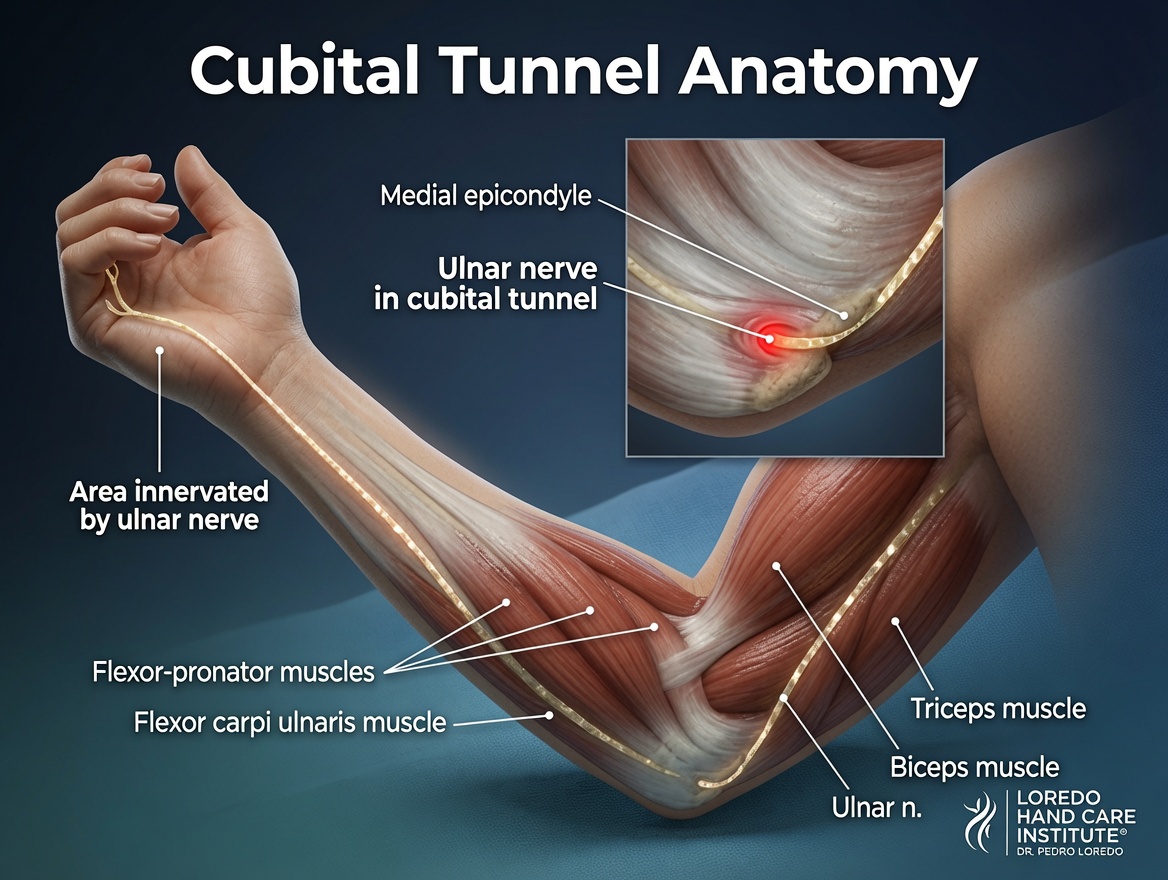
The cubital tunnel is a narrow passage on the medial side of the elbow where the ulnar nerve runs behind the bony bump (medial epicondyle). The roof of the tunnel is a fibrous band called Osborne's ligament. Just distal to the tunnel, the nerve passes between the two heads of the FCU muscle and beneath the deep fascia. Each of these structures can compress the nerve. Cubital tunnel syndrome is the second most common nerve compression in the upper extremity (after carpal tunnel) and produces numbness in the ring and small fingers, weak grip, and hand muscle wasting in advanced cases.
Endoscopic cubital tunnel release decompresses the nerve along its full length without moving it from its anatomic groove. A small endoscope is introduced through a single 2 cm incision and used to visualize and divide the compressing structures under direct view. The nerve remains in its native bed (in-situ release). For full background on the underlying condition, see Cubital Tunnel Syndrome.
Who Is a Candidate?
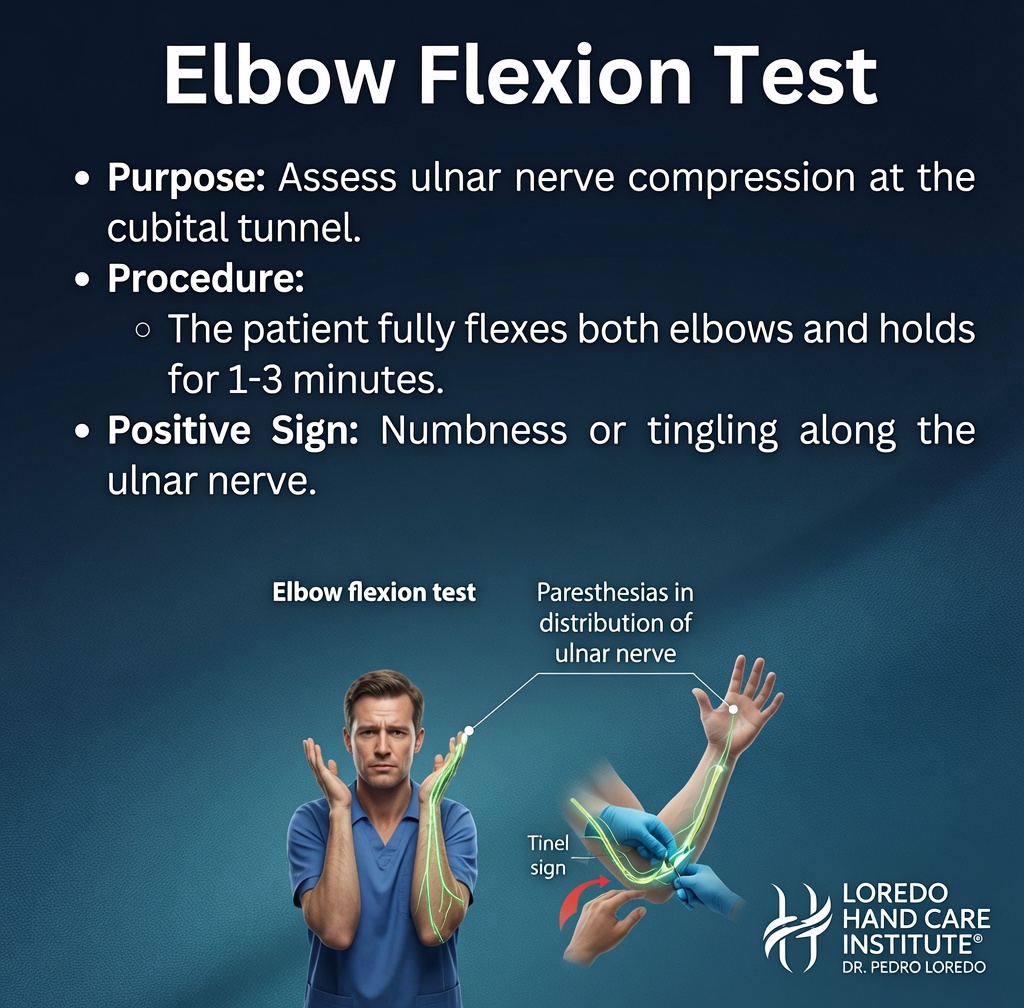
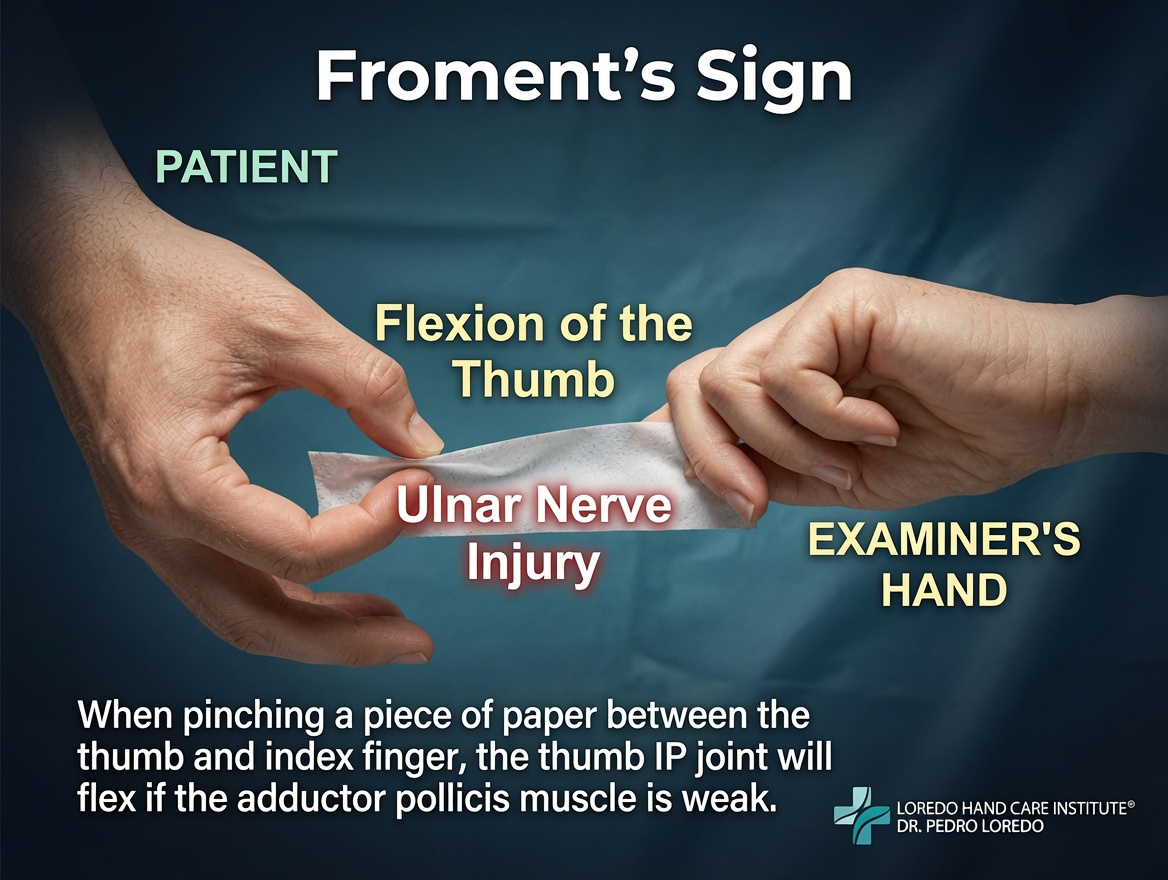
- Cubital tunnel syndrome confirmed by clinical examination, with positive Tinel sign at the elbow, positive elbow flexion test, or Froment's sign
- Electrodiagnostic studies (EMG and nerve conduction) confirming ulnar nerve slowing across the elbow
- Failure of 6 to 12 weeks of activity modification, night elbow extension splinting, and ergonomic correction
- Severe symptoms with constant numbness, hand muscle wasting, or grip weakness that warrant prompt release
- Patient preference for a minimally invasive approach with rapid recovery
Open in-situ release or anterior transposition (subcutaneous, intramuscular, or submuscular) may be preferred in certain cases: a subluxing nerve that snaps over the medial epicondyle with elbow flexion, prior elbow surgery, certain anatomic variants, or revision cases. Dr. Loredo discusses all options at consultation.
How the Procedure Is Performed
- Positioning and anesthesia. The patient lies supine with the affected arm extended on a hand table. Light intravenous sedation is given (MAC anesthesia). A local anesthetic block is placed at the elbow.
- Incision. A 2 cm posteromedial incision is made just behind the medial epicondyle, in the natural skin crease. The medial antebrachial cutaneous nerve branches are identified and protected.
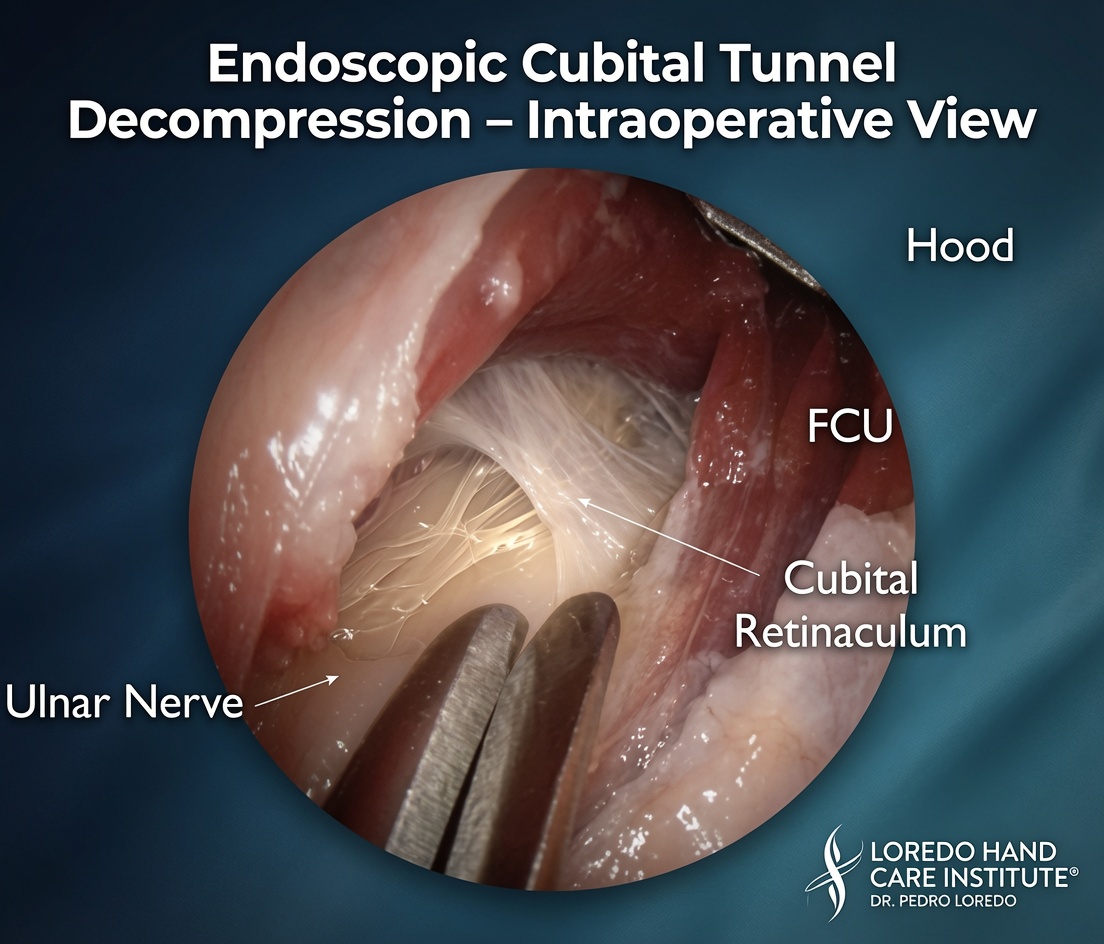
- Endoscope introduction. A specialized endoscope is introduced into the cubital tunnel and advanced both proximally and distally along the path of the ulnar nerve. The fiber-optic camera projects a magnified view onto a video monitor.
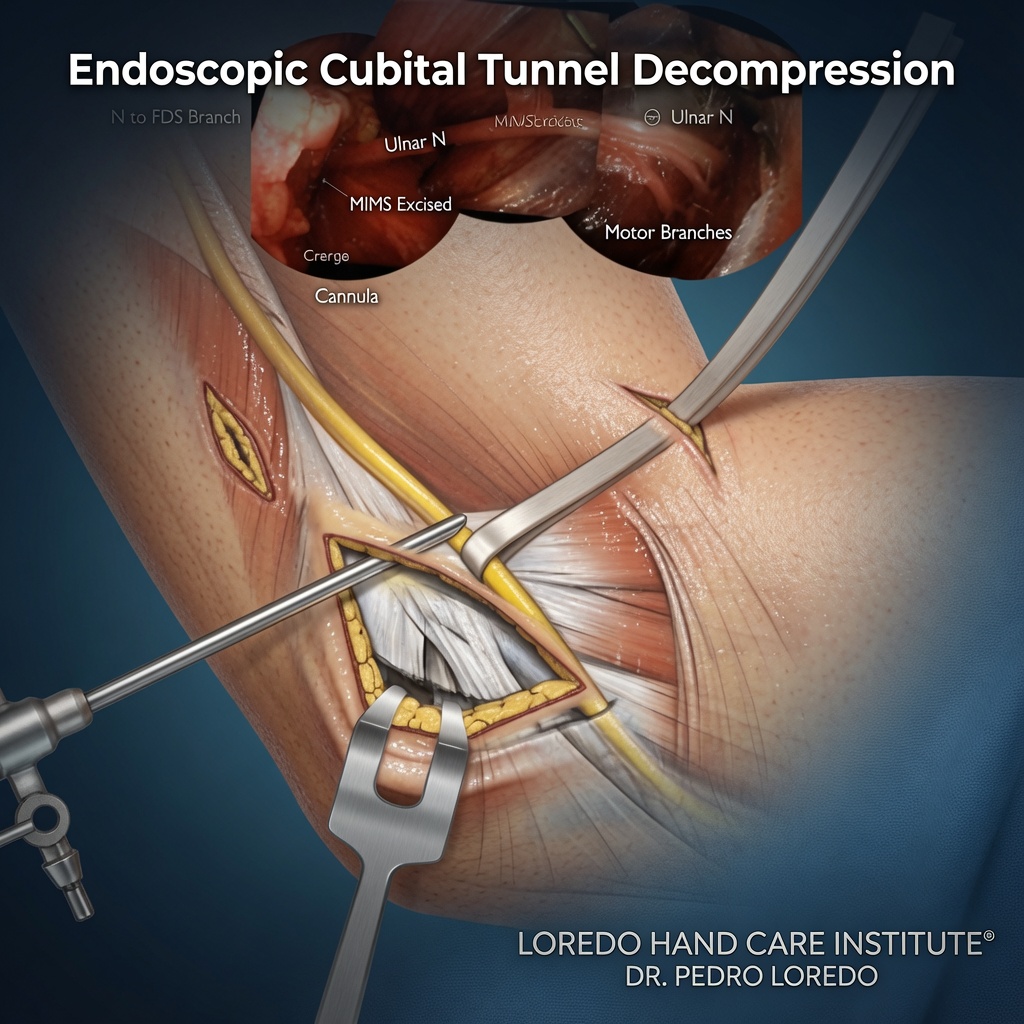
- Decompression. Under endoscopic visualization, the compressing structures are divided in sequence: the medial intermuscular septum proximally, Osborne's ligament at the cubital tunnel, the leading edge of the FCU muscle, and the deep flexor-pronator fascia distally. The nerve is decompressed for approximately 8 to 10 cm of its course.
- Confirmation and closure. The endoscope is removed and the release is confirmed by direct palpation. The skin is closed with a buried absorbable suture and adhesive strips.
- Dressing. A soft bulky dressing is applied. A sling is provided for comfort during the first 1 to 3 days.
Anesthesia Options
- MAC with local block (most common): light intravenous sedation plus local anesthetic at the elbow. You are comfortable and relaxed but breathing on your own.
- Bier block (regional intravenous anesthesia): the entire arm is numbed below a tourniquet. Used in selected cases.
- General anesthesia: rarely needed; reserved for patients who cannot tolerate sedation or who have specific medical considerations.
Procedure Duration and Setting
The actual surgical time is 30 to 60 minutes per elbow. Total time at the surgery center is 2 to 3 hours including check-in, anesthesia, the procedure, and recovery. The procedure is performed at an accredited ambulatory surgery center. Discharge is the same day. A family member or friend drives you home.
Recovery Timeline
- Day 0: Sling rest. Light hand and finger motion several times per day. Keep the dressing clean and dry.
- Day 1 to 5: Light activity at home. Pain typically peaks in the first 48 hours and improves substantially by day 5. Most patients are off pain medication by day 3 to 5.
- Week 1 to 2: First post-operative visit. Sling discontinued when comfortable. Begin gentle elbow range of motion. Most patients return to office work in this window.
- Week 2 to 6: Progressive elbow and hand strengthening. Hand therapy as needed for nerve gliding exercises.
- Week 6 to 12: Return to manual labor and athletic activity. Sensory recovery progressing.
- Months 3 to 12: Motor recovery continues in patients with significant pre-operative muscle wasting. Full strength may take up to a year.
Return to Work and Daily Activities
- Office or desk work: 1 to 2 weeks
- Light manual labor: 4 to 6 weeks
- Heavy manual labor and overhead work: 8 to 12 weeks
- Driving: 1 to 2 weeks once off pain medication and able to grip the wheel comfortably
- Sport with elbow loading (throwing, racquet sports, weightlifting): 3 to 4 months with progressive return
Why Endoscopic Matters
- Single 2 cm incision compared to 5 to 12 cm for open in-situ release or transposition
- Less postoperative pain and lower opioid requirements in the first week
- Smaller, more cosmetic scar hidden in the natural skin crease behind the medial epicondyle
- Faster return to function compared to transposition, which requires substantial soft-tissue dissection
- Lower risk of elbow stiffness than transposition
- Direct endoscopic visualization of the entire course of the ulnar nerve, ensuring complete release
Long-term symptom relief is comparable between endoscopic and open in-situ release. Anterior transposition may be preferred for nerve subluxation or specific revision cases, but is not necessary for most cubital tunnel syndrome.
Risks and Complications
Endoscopic cubital tunnel release is a safe procedure when performed by a fellowship-trained hand surgeon. Recognized risks include:
- Incomplete release (rare): the compression sites are not all divided. Symptoms persist or recur.
- Direct ulnar nerve injury (very rare): risk minimized by endoscopic visualization.
- Medial antebrachial cutaneous nerve injury: small risk of numbness in a patch of skin on the inner forearm; usually resolves over months.
- Hematoma: rare; treated with observation or rarely surgical drainage.
- Infection (less than 1 percent): treated with antibiotics.
- Nerve subluxation after release: in patients whose nerve was already partially subluxing pre-operatively, release alone may not stabilize it; transposition may be needed in revision.
- Persistent or recurrent symptoms: most often related to severe pre-operative compression with incomplete recovery rather than incomplete surgery.
- Anesthesia-related risks: rare with MAC sedation.
Cost and Insurance
Endoscopic cubital tunnel release (CPT 64718) is covered by virtually all commercial insurance plans, Medicare, the VA Community Care Network under the MISSION Act, and Texas workers' compensation when the diagnosis is appropriately documented. The total cost includes the surgeon fee, the surgery center facility fee, and the anesthesia fee. Out-of-pocket cost depends on your specific plan, deductible, and copay. Our team verifies your benefits before surgery and provides a clear estimate. Call our office at (972) 939-4974 for a benefits check before your visit.
Frequently Asked Questions
How is endoscopic cubital tunnel release different from open in-situ release or transposition?
Open in-situ release uses a longer incision (5 to 8 cm) along the medial elbow to expose and decompress the ulnar nerve. Anterior transposition moves the nerve from behind the medial epicondyle to a position in front of it, typically through a 10 to 12 cm incision. Endoscopic release uses a single 2 cm incision and decompresses the nerve along its full length under direct endoscopic visualization without moving it. The endoscopic approach has less postoperative pain, faster return to function, and lower elbow-related complication rates than transposition. Long-term symptom relief is comparable to open in-situ release for most patients.
How long does the procedure take?
The actual surgical time is 30 to 60 minutes. Add about 60 minutes for check-in, anesthesia, dressing, and recovery before discharge. Patients typically arrive 90 minutes before the scheduled surgery time and leave the surgery center 2 to 3 hours after arrival.
Will my hand strength come back?
Sensory recovery is typically good and progresses over 6 to 12 weeks. Motor recovery is more variable and depends on how long the nerve was compressed and how severe the muscle wasting was before surgery. Mild to moderate cases recover near-normal strength. Severe cases with visible thinning of the small hand muscles may have permanent weakness even after a successful decompression. Earlier surgery leads to more complete recovery.
When can I drive and return to work?
Most patients drive within 1 to 2 weeks after endoscopic cubital tunnel release, once they are off pain medication and can grip the steering wheel comfortably. Office or desk work resumes 1 to 2 weeks after surgery. Manual labor and heavy lifting return at 4 to 6 weeks, often through a brief light-duty period. Driving and return-to-work timing after open transposition is typically 1 to 2 weeks longer.
Can this be performed at the same time as carpal tunnel release?
Yes. Patients with both ulnar nerve compression at the elbow and median nerve compression at the wrist (a recognized double crush pattern) can have both procedures performed in the same operating session through separate small incisions. Combined surgery avoids two anesthetic exposures and shortens total recovery.
Related Conditions
- Cubital Tunnel Syndrome: the underlying condition this procedure treats.
- Guyon's Canal Syndrome: ulnar nerve compression at the wrist. Differentiated by the presence of dorsal hand numbness.
- Golfer's Elbow: medial epicondylitis. Frequently coexists with cubital tunnel syndrome and can be addressed in the same operative setting.
- Carpal Tunnel Syndrome: the recognized double crush partner. Often released in the same session.
Related Procedures
- Endoscopic Carpal Tunnel Release: the wrist counterpart, often performed in the same session.
- Microsurgery: peripheral nerve repair and revision when the nerve has been previously injured.
- All Procedures: the full list of surgical procedures offered at the practice.
From the Blog
- Cubital Tunnel Surgery Recovery: day-by-day post-op timeline.
- What Minimally Invasive Really Means: endoscopic versus open ulnar nerve decompression.
- The Ulnar Nerve and Why It Matters: anatomy and the three main compression sites.
Watch: Endoscopic cubital tunnel release education
Short videos from Dr. Loredo's Instagram and Facebook channels.