Microsurgery is a category of hand surgery performed under the operating microscope at 10x to 40x magnification. The technique is required when the structures being repaired or reconstructed are too small or too delicate for standard loupe magnification. Dr. Loredo offers the full range of upper extremity microsurgery: peripheral nerve repair after laceration, nerve grafting and nerve transfer for chronic nerve injuries, microvascular vessel repair and bypass for ischemic injuries, digit replantation after traumatic amputation, free tissue transfer (free flaps) for soft tissue reconstruction after trauma or tumor resection, and microsurgical sympathectomy for severe Raynaud's. Dr. Loredo trained in microsurgery at the Kleinert and Kutz Hand Care Institute and assisted on a hand transplant during his fellowship at the Christine M. Kleinert Institute in Louisville, Kentucky.
What Is Microsurgery?
Microsurgery is surgery performed under high-magnification with specialized instruments that match the scale of the structures being operated on. The operating microscope provides 10x to 40x magnification of the surgical field. Sutures used range from 8-0 (about 0.04 mm in diameter) for medium vessels to 10-0 (about 0.02 mm) for tiny vessels and peripheral nerve fascicles. The instruments are scaled accordingly: forceps, scissors, and needle holders are precision tools that fit the operator's hand but work at submillimeter scale.
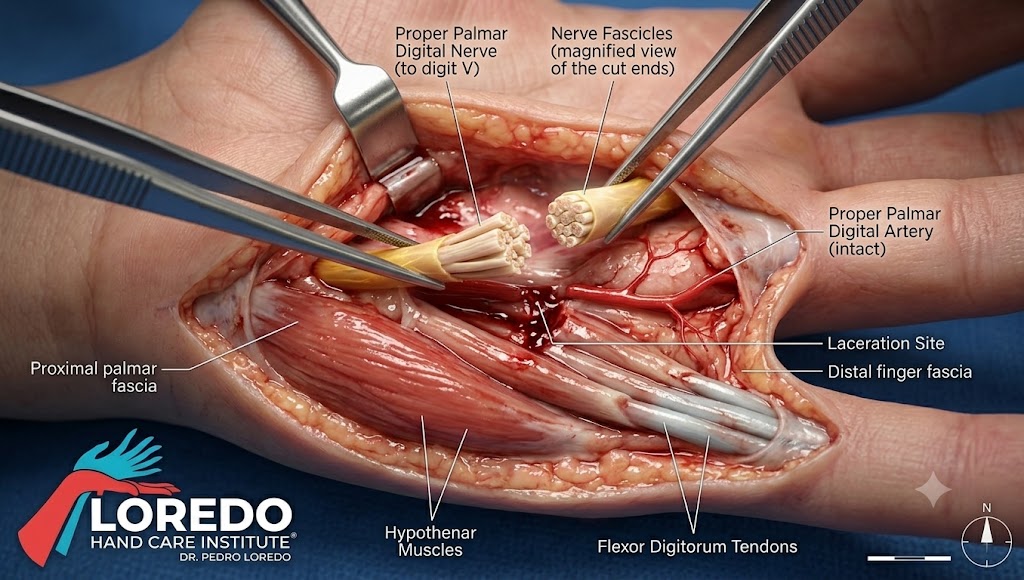
Microsurgery is required when standard loupe magnification (typically 2.5x to 4.5x) is insufficient. Peripheral nerves contain hundreds of microscopic fascicles that must be aligned for accurate repair. Digital arteries are 1 to 2 mm in outer diameter with walls thinner than a sheet of paper. Successful repair of these structures depends on the ability to see and manipulate them at the appropriate scale.
Categories of Microsurgical Procedures
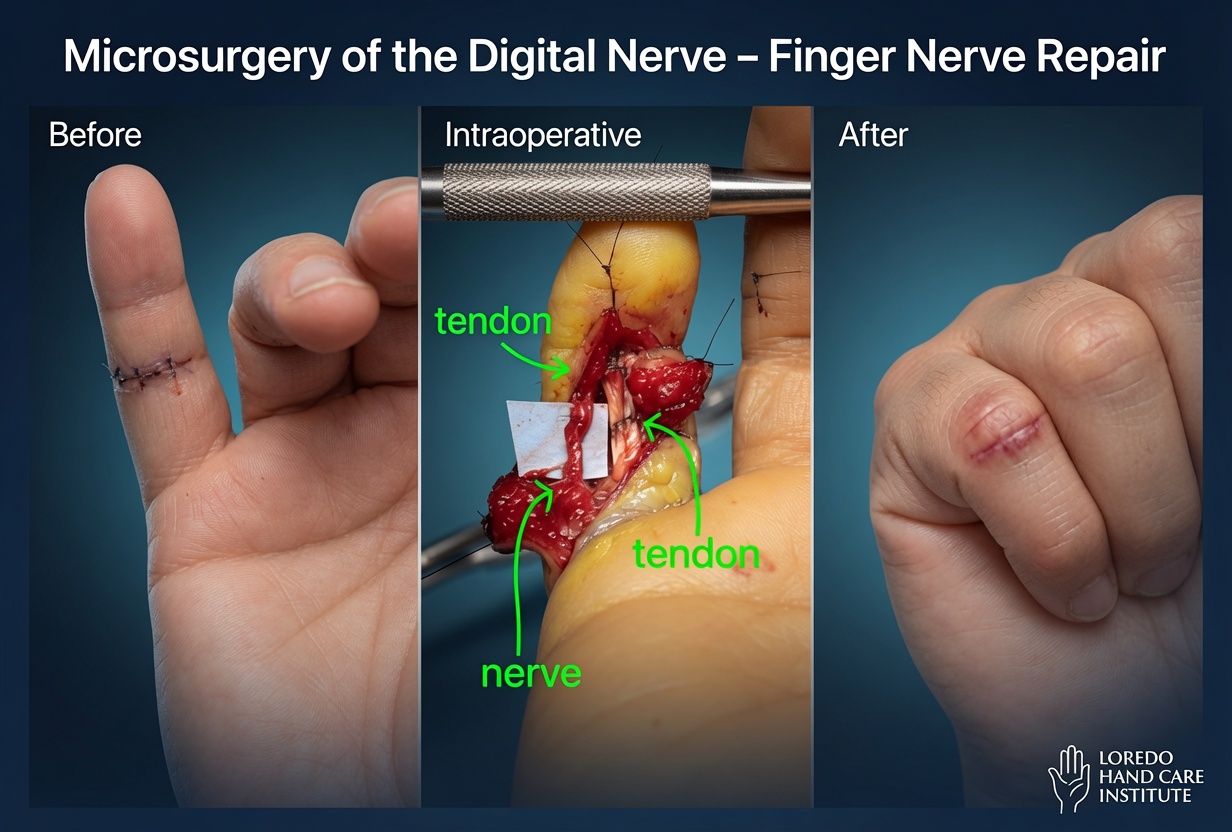
Peripheral Nerve Repair
Direct microsurgical reattachment of a cut nerve. Performed within hours to days of the injury when possible. The proximal and distal ends are aligned under microscope, and 8 to 12 fine sutures (9-0 or 10-0 nylon) are placed in the epineurium (outer nerve sheath) to bring the ends together without tension. Recovery is paced by nerve regeneration: approximately 1 mm per day from the repair site to the muscle or sensory end-organ.
Nerve Grafting and Nerve Transfer
For chronic injuries or when direct repair is not possible because of a nerve gap, a graft (typically the sural nerve from the leg) bridges the gap. Nerve transfers redirect a working nerve to power a paralyzed muscle, useful in upper extremity nerve injuries when proximal repair is not feasible.
Microvascular Vessel Repair
Direct repair of a cut artery or vein. Used in revascularization of an ischemic finger or hand, in flap surgery to connect the flap blood supply to recipient vessels, and in replantation. Requires patient and methodical microsurgical technique with 9-0 or 10-0 nylon sutures placed circumferentially around the vessel.
Digit Replantation
Microsurgical reattachment of an amputated finger, thumb, hand, or arm. The procedure requires bone fixation, tendon repair, microvascular artery and vein repair, microsurgical nerve repair, and skin closure. Operating time is 4 to 8 hours per digit. Postoperative monitoring is intensive: 5 to 7 days inpatient, with strict no-smoking, no-caffeine, warm-room protocols to maintain blood flow through the small repaired vessels. Success depends on the level of amputation, mechanism, ischemia time, and patient factors.
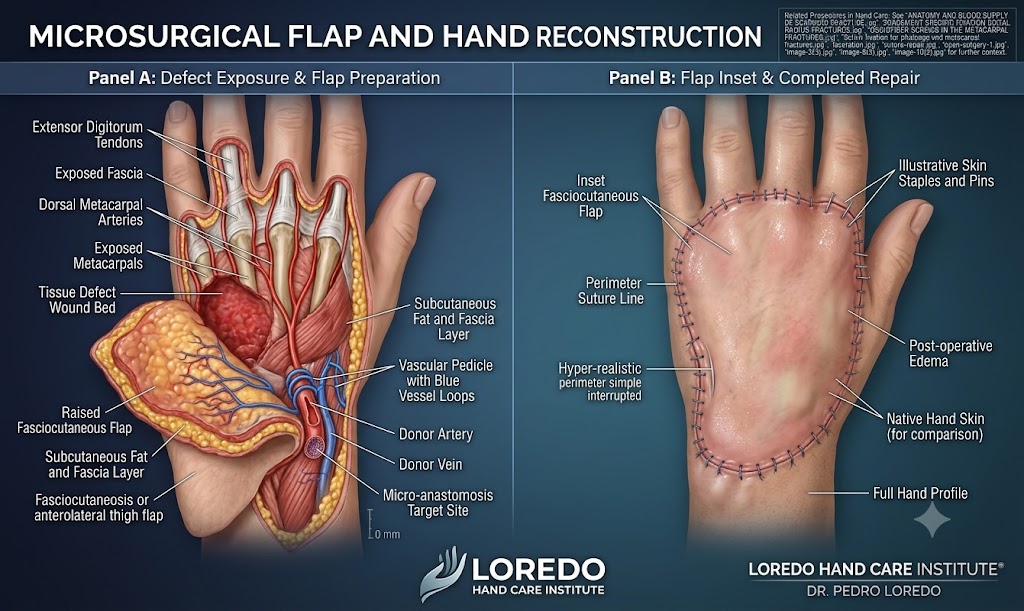
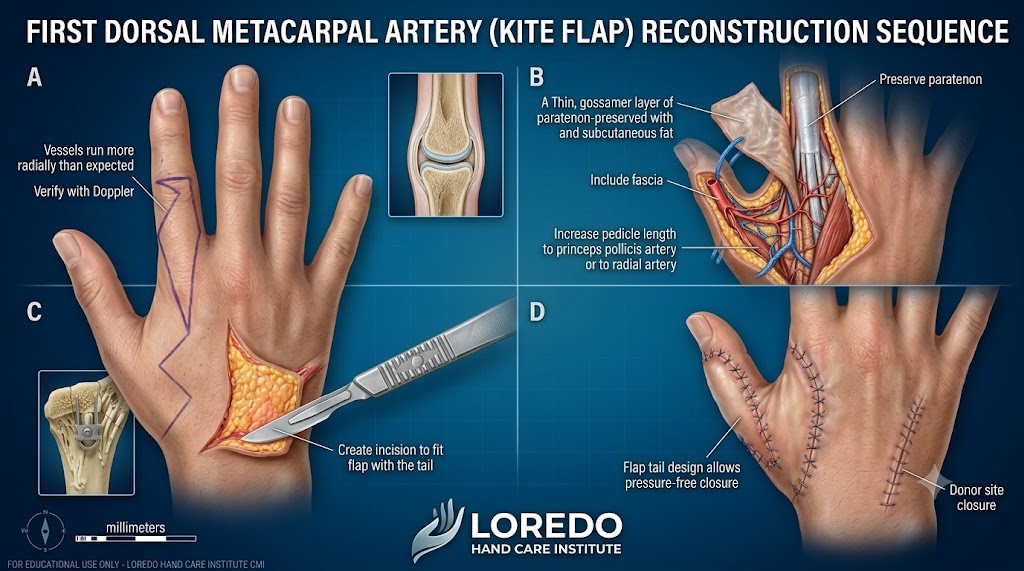
Free Tissue Transfer (Free Flap)
Transfer of a block of tissue (skin, muscle, or composite) with its own blood supply from one part of the body to another to reconstruct a defect. The donor vessels are connected to recipient vessels at the new location using microsurgical technique. Used for large soft tissue defects after trauma, tumor resection, or chronic wounds.
Microsurgical Sympathectomy
For severe refractory Raynaud's with digital ulcers or threatened tissue loss. The sympathetic nerve fibers traveling along the digital arteries are stripped under microscope, eliminating the signal that drives vasospasm. See the Raynaud's Disease page for full discussion.
Who Is a Candidate?
- Acute peripheral nerve laceration of the hand or upper extremity
- Chronic peripheral nerve injury with persistent neurologic deficit
- Acute amputation of a digit, thumb, hand, or upper extremity
- Vascular injury threatening tissue viability in the hand
- Soft tissue defect requiring free flap reconstruction
- Severe refractory Raynaud's with digital ulcers (microsurgical sympathectomy)
- Failed previous nerve repair requiring revision or grafting
How a Microsurgical Procedure Is Performed
- Pre-operative planning: imaging, examination, and identification of donor and recipient sites for grafts or flaps. Acute injuries are evaluated emergently.
- Anesthesia: regional or general, depending on procedure. Replantation and free flap surgery typically use general anesthesia.
- Surgical exposure: incisions appropriate to the structures being repaired or transferred.
- Microscope setup: the operating microscope is positioned over the surgical field. Magnification is increased from 6x to 40x as needed.
- Microsurgical repair: nerve fascicles or vessel walls are approximated with fine sutures under microscope. Patency is confirmed with vessel filling or nerve continuity testing.
- Closure: standard wound closure with attention to soft tissue coverage of the repair site.
- Postoperative monitoring: variable by procedure. Replantation and free flap require continuous flap monitoring for 3 to 5 days.
Anesthesia Options
- Regional block (axillary, supraclavicular, or interscalene): the entire arm is numbed for several hours, often with a continuous catheter for 1 to 3 days.
- General anesthesia: standard for replantation and free flap surgery.
- Combined regional plus light sedation: for shorter microsurgical cases.
Procedure Duration and Setting
Microsurgical procedures range widely in duration and setting:
- Single peripheral nerve repair: 1 to 2 hours, ambulatory surgery center, same-day discharge.
- Digit replantation: 4 to 8 hours per digit, hospital, 5 to 7 days inpatient.
- Free flap reconstruction: 4 to 10 hours, hospital, 3 to 7 days inpatient.
- Microsurgical sympathectomy: 1 to 2 hours per finger, ambulatory surgery center.
Recovery Timeline
Recovery is highly variable depending on the procedure.
- Peripheral nerve repair: immobilization 2 to 4 weeks, then progressive motion. Sensory and motor recovery follows nerve regeneration at approximately 1 mm per day from the repair site. Full recovery 6 to 24 months depending on the level of injury.
- Digit replantation: inpatient monitoring 5 to 7 days. Splinting 4 to 6 weeks. Hand therapy 3 to 6 months. Sensory and functional recovery progresses over 1 to 2 years. Replanted digits are typically stiffer and less sensate than uninjured digits but functional.
- Free flap: inpatient monitoring 3 to 7 days. Wound and donor site healing 4 to 6 weeks. Functional recovery depends on the recipient site.
- Sympathectomy: dressing 1 week, gentle motion at 2 weeks, full activity 4 to 6 weeks.
Returning to Work and Daily Activities
Highly variable. After single nerve repair, office work returns in 1 to 2 weeks; manual labor in 6 to 12 weeks. After replantation, return to work depends on dominant versus non-dominant hand, occupation, and recovery progress; typically 3 to 6 months for office work and 6 to 12 months for manual labor. After free flap, donor site recovery can be the rate-limiting step.
Why Specialized Training Matters
Microsurgery requires dedicated fellowship training. The technical skill is acquired over months to years of supervised practice with the microscope. Dr. Loredo completed his Hand and Upper Extremity Surgery Fellowship at the Christine M. Kleinert Institute (2007 to 2008), with dedicated microsurgery training at the Kleinert and Kutz Hand Care Institute (December 2007 to January 2008). The Kleinert programs are internationally recognized as the foundational institutions in modern hand microsurgery. During his fellowship Dr. Loredo assisted on a hand transplant at the Kleinert Kutz Hand Care Institute.
Risks and Complications
- Failed repair: nerve or vessel repair does not heal. May require revision or alternative reconstruction.
- Replantation failure: 10 to 30 percent of replanted digits fail to maintain blood flow despite optimal technique. Revision amputation may be needed.
- Free flap failure: 5 to 10 percent of free flaps fail and require revision or alternative reconstruction.
- Donor site morbidity after nerve grafting (sural nerve graft) or free flap (variable depending on donor site).
- Stiffness after replantation and complex hand reconstruction is common; hand therapy mitigates this.
- Complex regional pain syndrome (CRPS): rare but recognized after major hand trauma.
- Standard surgical risks: bleeding, infection, anesthesia-related complications.
Cost and Insurance
Microsurgical procedures are covered by virtually all commercial insurance plans, Medicare, the VA Community Care Network, and Texas workers' compensation when medically indicated. Acute trauma cases are evaluated and treated as emergencies regardless of insurance status; financial counseling occurs after stabilization. For elective microsurgical procedures (chronic nerve repair, sympathectomy), our team verifies benefits before surgery. Call our office at (972) 939-4974 for a benefits check.
Frequently Asked Questions
What kinds of microsurgery does Dr. Loredo perform?
Dr. Loredo performs the full range of microsurgical procedures on the hand and upper extremity: primary peripheral nerve repair after laceration, nerve grafting and nerve transfer for chronic injuries, microvascular vessel repair and bypass for ischemic injuries, digit replantation after traumatic amputation, free tissue transfer (flaps) for soft tissue reconstruction after trauma or tumor resection, and microsurgical sympathectomy for severe Raynaud's. The unifying technical element is the use of an operating microscope at 10x to 40x magnification with microsurgical instruments and 8-0 to 10-0 sutures.
What is Dr. Loredo's microsurgery training?
Dr. Loredo completed his Hand and Upper Extremity Surgery Fellowship at the Christine M. Kleinert Institute, University of Louisville (2007-2008), with dedicated microsurgery training at the Kleinert and Kutz Hand Care Institute (December 2007 to January 2008). During this fellowship he assisted on a hand transplant at the Kleinert Kutz Hand Care Institute, one of a small number of hand transplants performed in the United States. The Kleinert programs are internationally recognized as the foundational institutions in modern hand microsurgery.
How long does it take a nerve to recover after repair?
Nerve regeneration progresses at approximately 1 mm per day after repair. The distance from the repair site to the muscle or sensory end-organ determines how long full recovery takes. A laceration at the wrist that requires regrowth to the fingertip is roughly 30 cm, which takes about 10 to 12 months of regeneration after repair. A more proximal injury at the elbow takes 18 to 24 months. Recovery is also influenced by patient age (younger nerves regrow faster), the time delay between injury and repair (earlier is better), the quality of repair, and the specific nerve. Hand therapy through the recovery period is essential.
What does digit replantation involve?
Replantation is the microsurgical reattachment of an amputated digit, hand, or arm. The procedure requires immediate evaluation, surgical exploration, microvascular reattachment of the arteries and veins, microsurgical nerve repair, tendon repair, and bone fixation. Total operating time is 4 to 8 hours per digit. Postoperative care includes 5 to 7 days of inpatient monitoring with strict no-smoking, no-caffeine, warm-room protocols to maintain blood flow. Success depends on the level of amputation (more distal is better), the mechanism (clean cut better than crush), the warm and cold ischemia times, and patient factors. Not every amputation is replantable; the surgeon makes that decision after immediate evaluation.
Is microsurgery available as an emergency?
Yes. Acute amputation, severe vascular injury with threatened tissue loss, and complex open hand trauma require emergency microsurgical evaluation, ideally within 6 hours for replantation candidacy. Patients who arrive at an emergency department with these injuries should request hand surgeon consultation immediately. Our office coordinates emergency consultations and accepts transfers for microsurgical care. The amputated part should be wrapped in saline-moistened gauze, placed in a sealed plastic bag, and the bag placed on ice (do not freeze the part directly) during transport.
Related Conditions
- Flexor Tendon Injury: complex flexor tendon injuries with associated nerve or vessel laceration require microsurgical repair.
- Extensor Tendon Injury: severe dorsal hand trauma may require microsurgical free flap coverage.
- Hand and Finger Fractures: open fractures with nerve or vessel injury require combined microsurgical and bone fixation.
- Raynaud's Disease: severe refractory Raynaud's with digital ulcers may benefit from microsurgical sympathectomy.
- Workers' Compensation Injuries: workplace amputations and complex hand trauma are common microsurgical referrals.
Related Procedures
- Hand Fracture Fixation: combined with microsurgical nerve and vessel repair in open fractures.
- Endoscopic Cubital Tunnel Release: peripheral nerve decompression that may be combined with microsurgical revision in complex cases.
- All Procedures: the full list of surgical procedures offered at the practice.
From the Blog
- Mallet Finger and Jersey Finger: When to Worry: small tendon injuries that may need microsurgical repair.
- Hand Therapy After Surgery: Certified Hand Therapist coordination after microsurgery.
Watch: Microsurgery education
Short videos from Dr. Loredo's Instagram and Facebook channels.