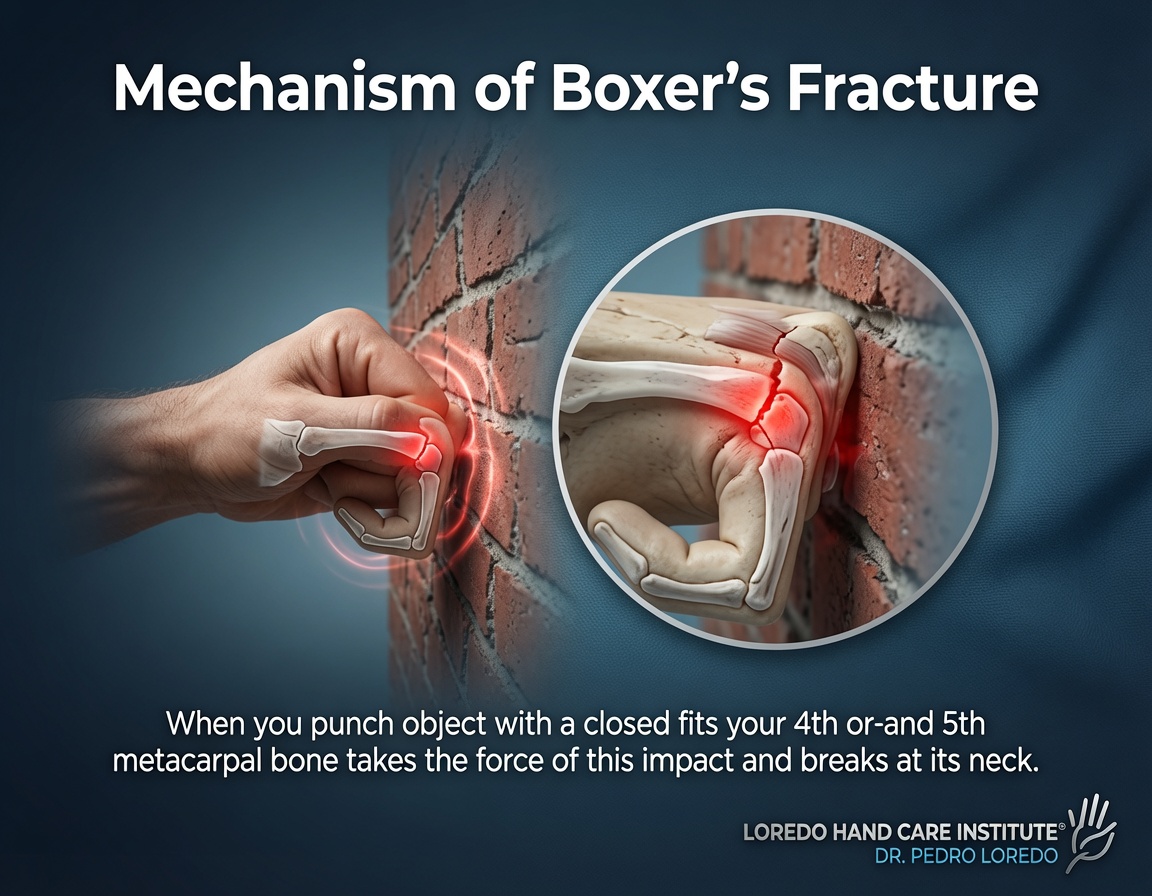
Hand fracture fixation covers the full range of techniques for treating displaced and unstable fractures of the hand and wrist. Method is matched to the fracture pattern: stable nondisplaced fractures get a cast or splint, displaced but reducible fractures often get closed reduction with percutaneous K-wire pinning, comminuted or intra-articular fractures usually need open reduction with internal fixation (ORIF) using plates and screws, and severely contaminated open fractures often start with external fixation. Common patterns Dr. Loredo treats include distal radius fractures (typically with a volar locking plate), scaphoid fractures (often with a percutaneous compression screw), 5th metacarpal neck fractures (boxer's, often K-wire pinning), and phalanx fractures (variable). Recovery depends on bone and method, with most patients in a cast or splint for 3 to 6 weeks, hand therapy for 6 to 12 weeks, and full strength returning at 8 to 16 weeks.
What Is Hand Fracture Fixation?
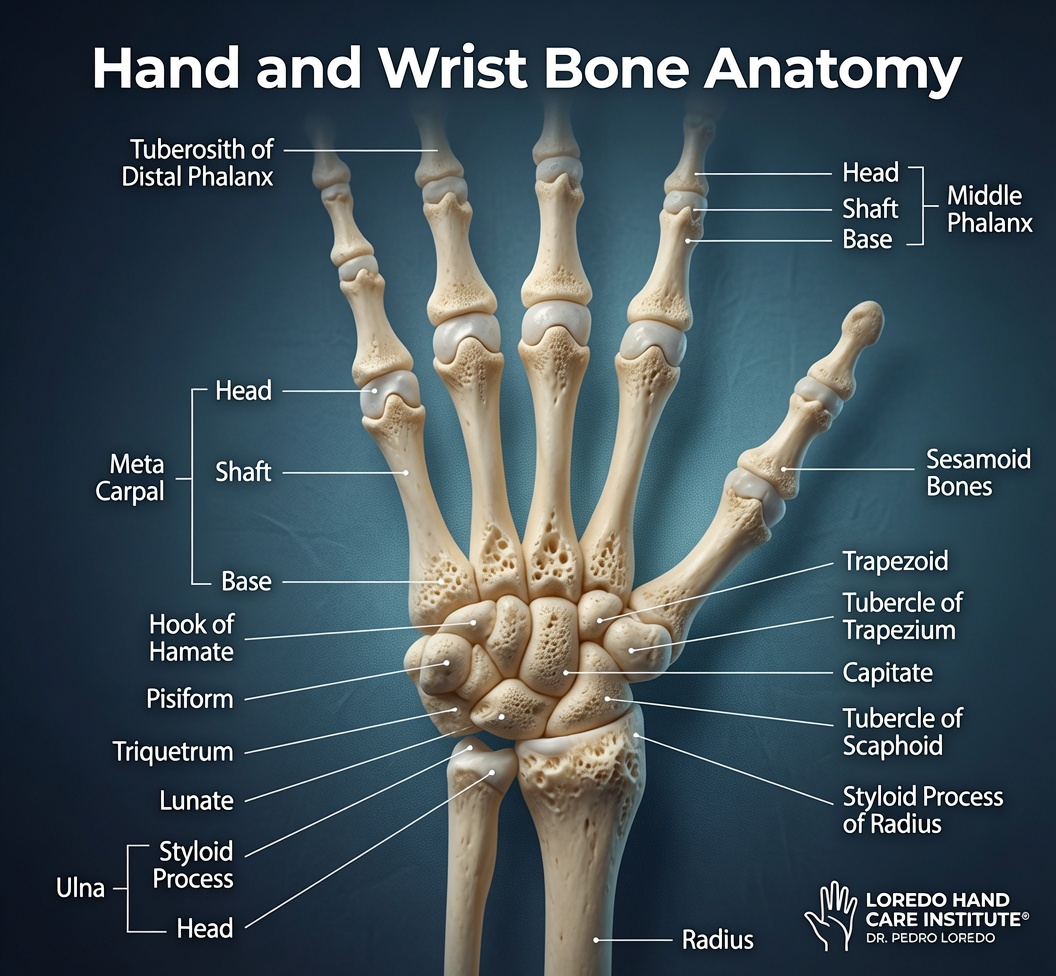
The hand and wrist contain 27 bones, and any of them can break. The goal of treatment is the same in every case: restore anatomic alignment, allow the bone to heal, and preserve hand function. The method used to achieve those goals depends on whether the fracture is stable or unstable, whether it involves a joint surface, whether it is displaced and how easily it can be reduced, the soft-tissue condition, and the patient's hand demands.
Most hand fractures are treated nonoperatively with cast or splint immobilization. A meaningful minority require surgical fixation to ensure the bone heals in correct anatomic position. The fixation method is matched to the fracture pattern. For full background on the underlying injuries, see Hand and Finger Fractures.
Who Is a Candidate?
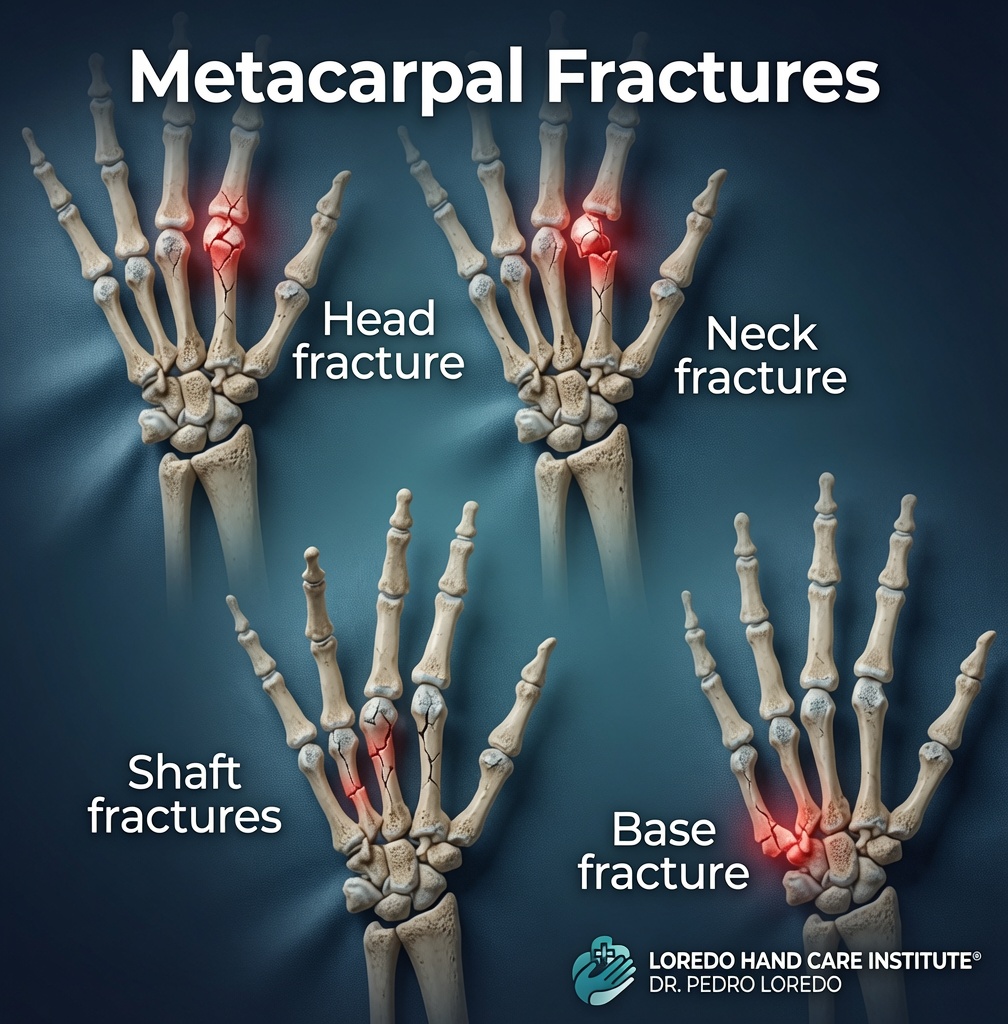
- Displaced fracture of the distal radius, metacarpal, or phalanx that does not maintain reduction in a cast
- Comminuted fracture (multiple bone fragments) that cannot be held with closed methods alone
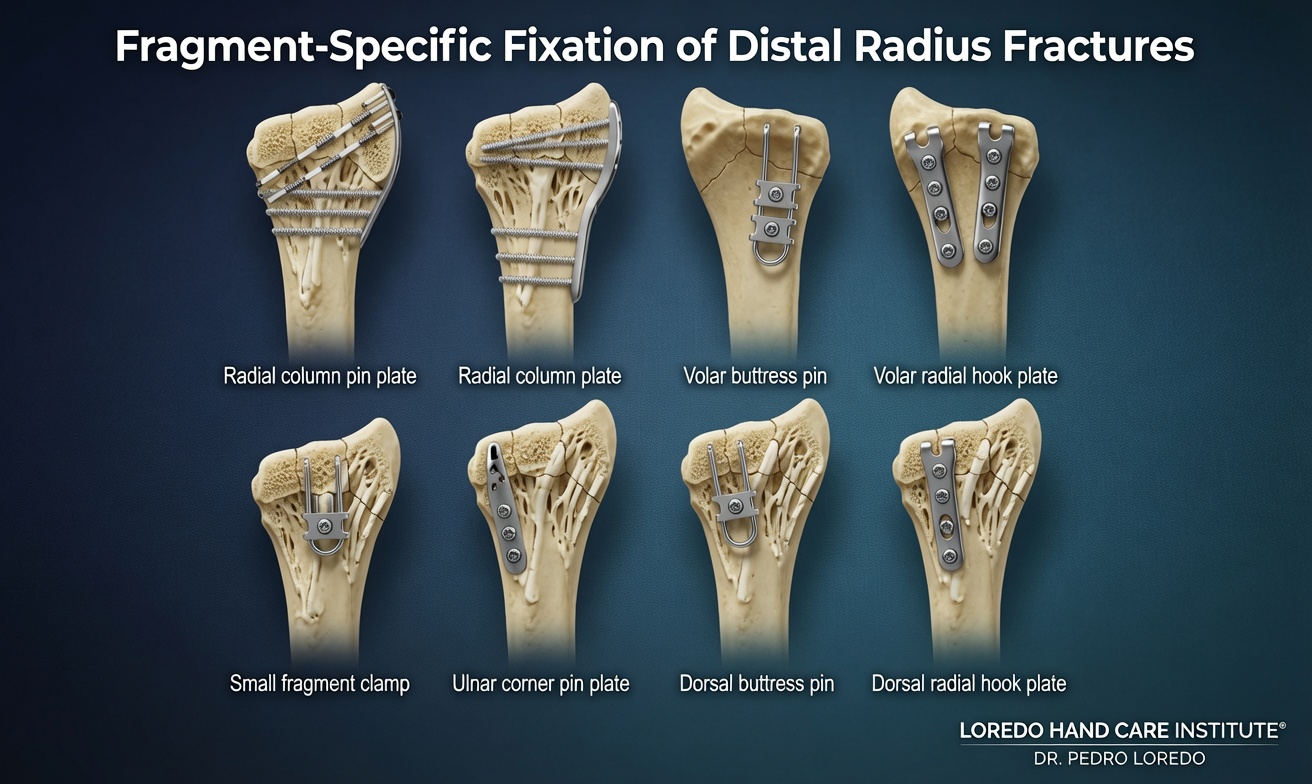
- Intra-articular fracture (involving the joint surface) requiring anatomic restoration
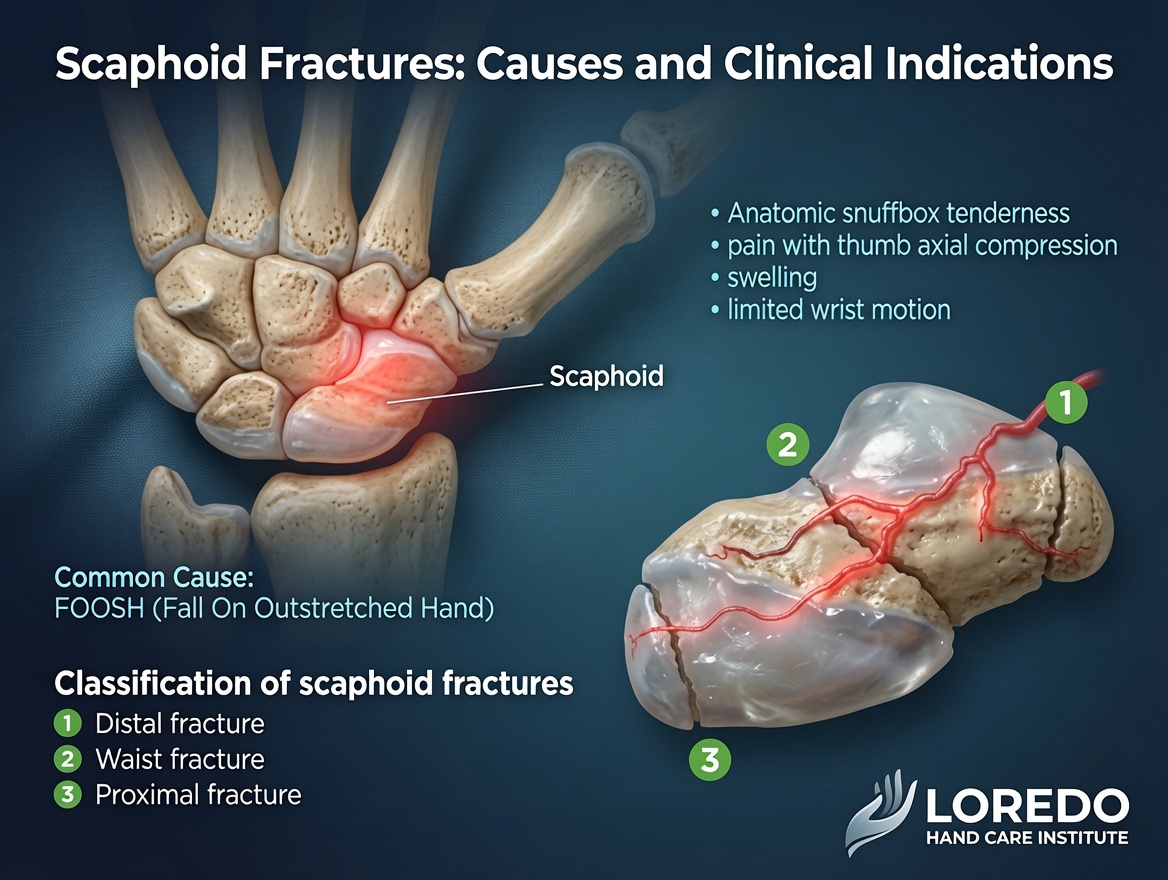
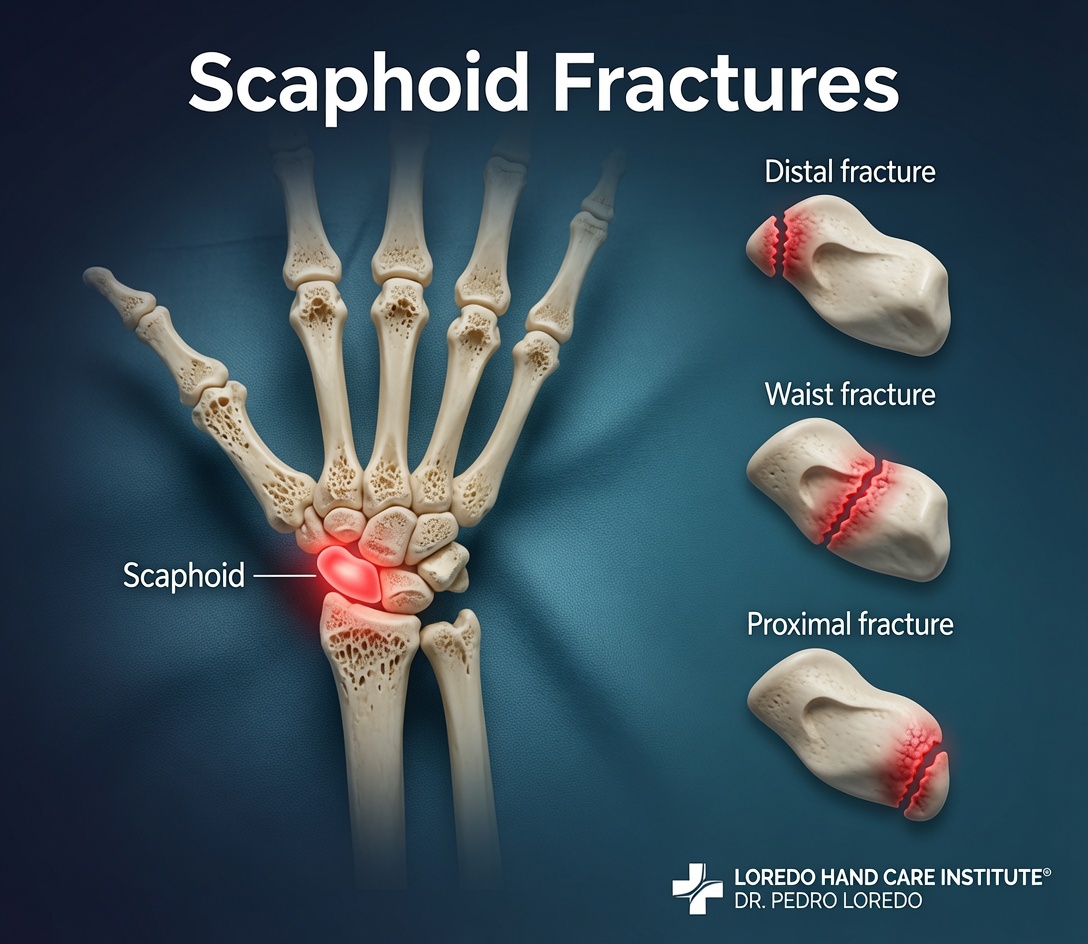
- Scaphoid fracture, particularly proximal pole or displaced waist fractures
- Open fracture with bone exposed through skin
- Rotational malalignment causing finger overlap when making a fist
- High-demand hand user (manual laborer, athlete, musician) who needs faster recovery than closed treatment provides
- Failed closed reduction with loss of position in a cast
- Malunion or nonunion from a prior poorly healed fracture
Fixation Methods
Closed Reduction with Cast or Splint
The simplest treatment. Stable nondisplaced or minimally displaced fractures heal well in a properly applied cast or splint. Displaced fractures are reduced under local or hematoma block anesthesia and then immobilized. The fracture is X-rayed at 1 to 2 weeks to confirm maintained alignment. If alignment is lost, conversion to surgical fixation is appropriate.
Percutaneous Pinning (K-wires)
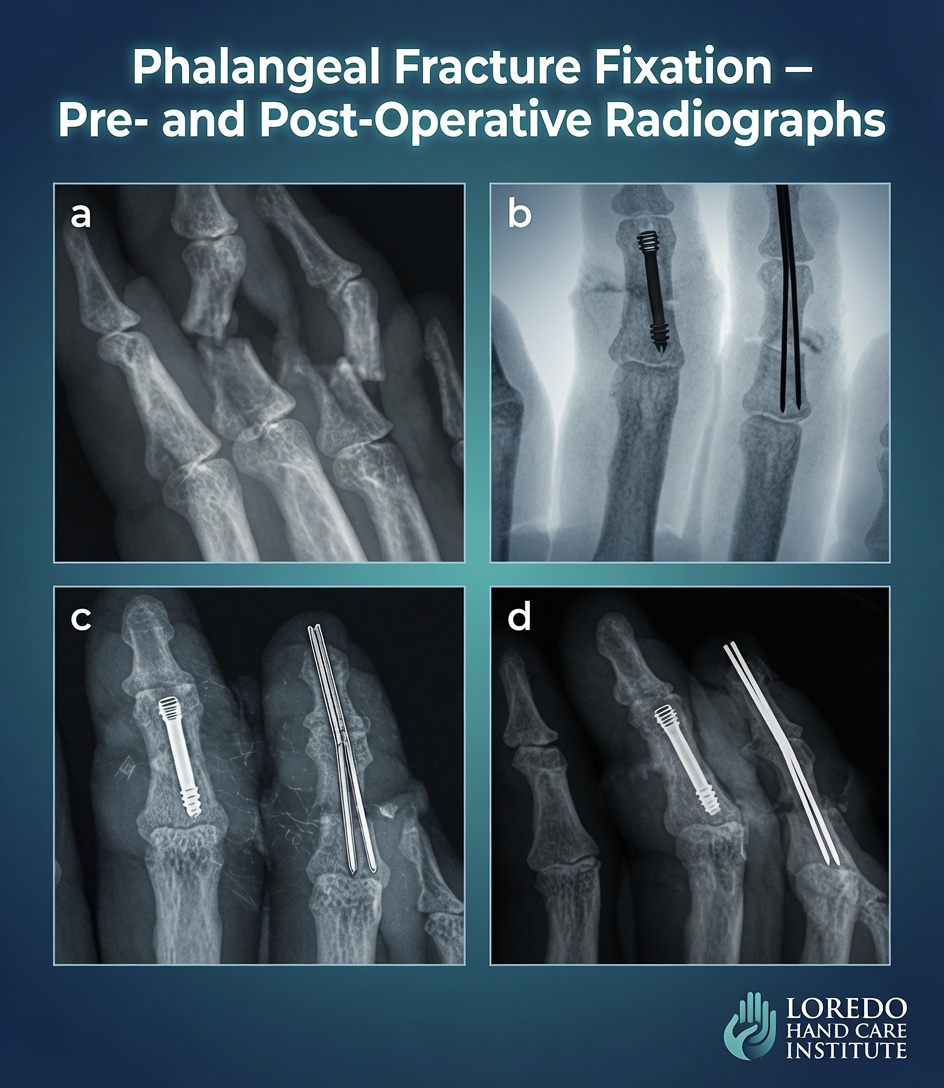
K-wires are smooth stainless-steel pins driven through small skin punctures into the bone to hold the fracture in alignment. Used for displaced but easily reducible fractures, particularly metacarpal and phalanx fractures, certain distal radius patterns, and selected scaphoid fractures. Pins are typically left protruding through the skin for 4 to 6 weeks and then removed in the office. Less invasive than open surgery; useful in young patients and certain fracture patterns.
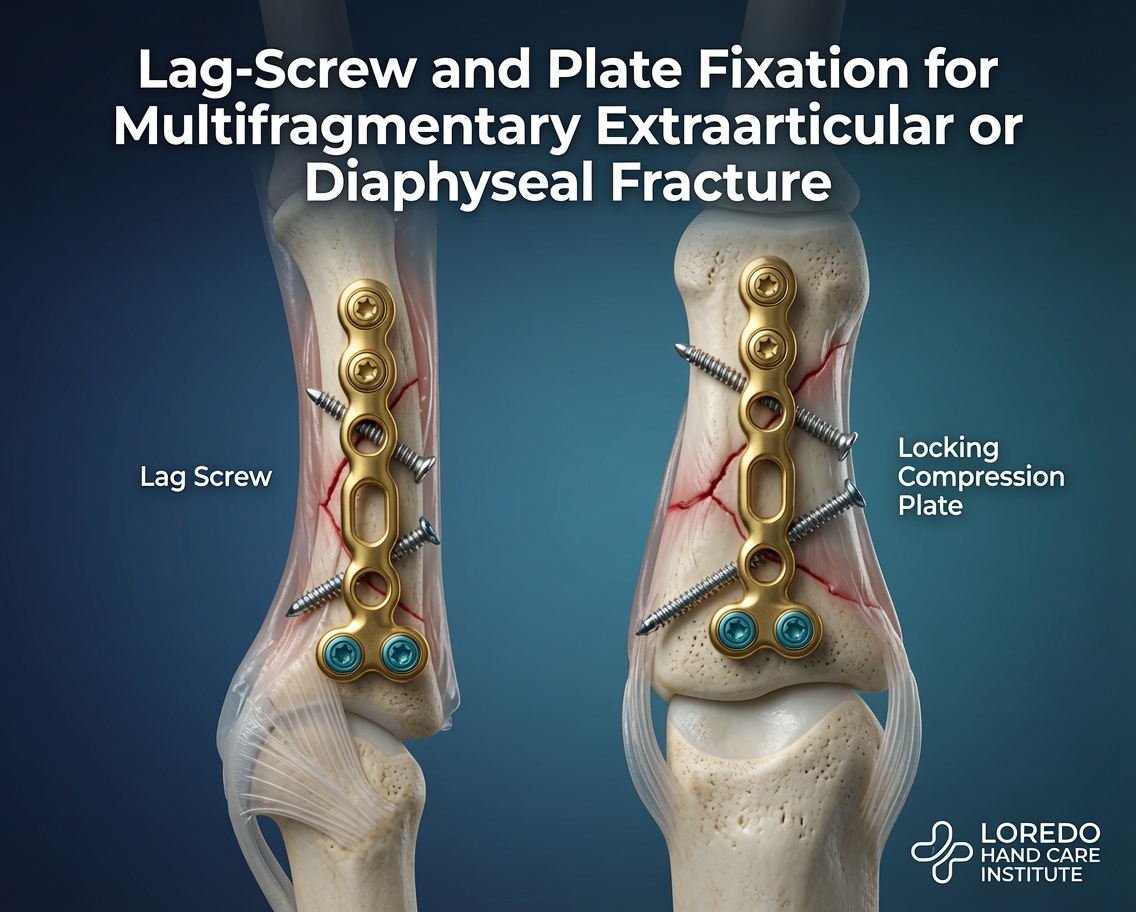
Open Reduction Internal Fixation (ORIF)
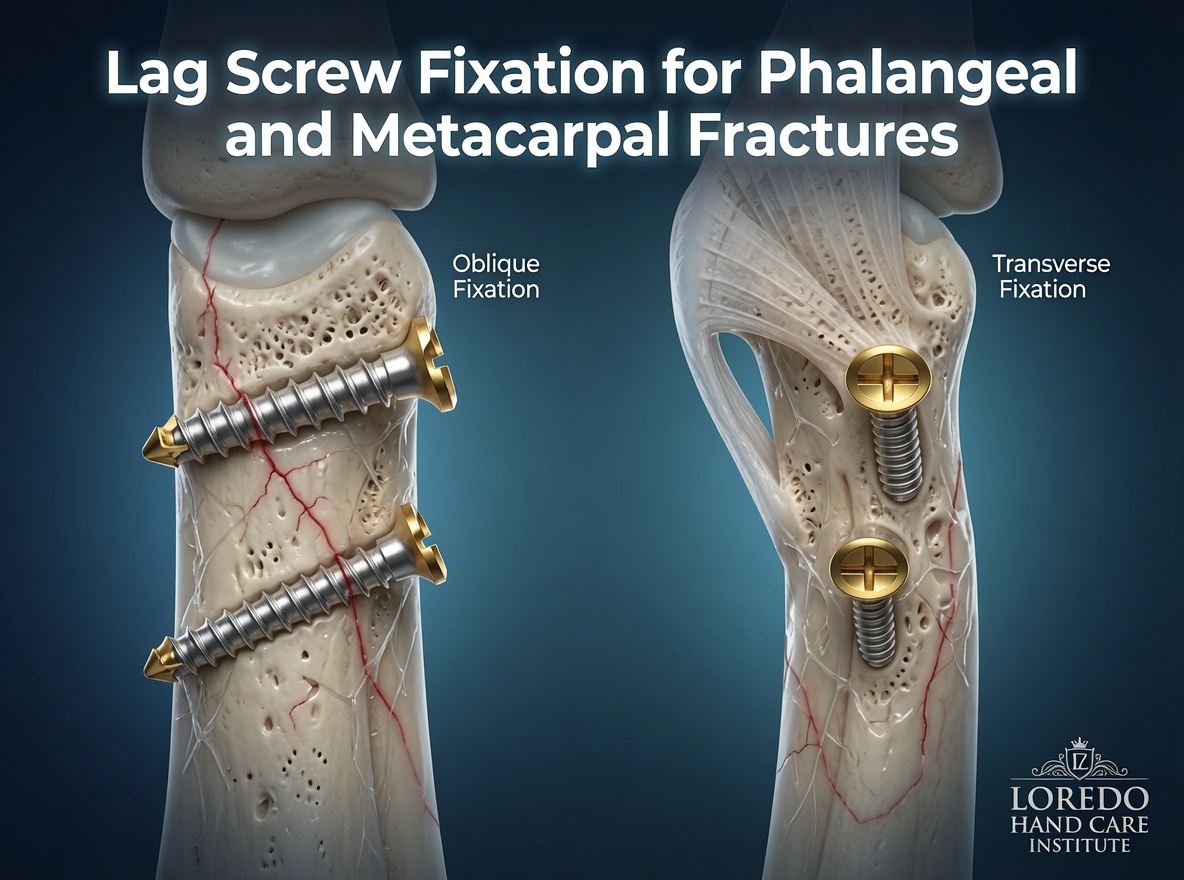
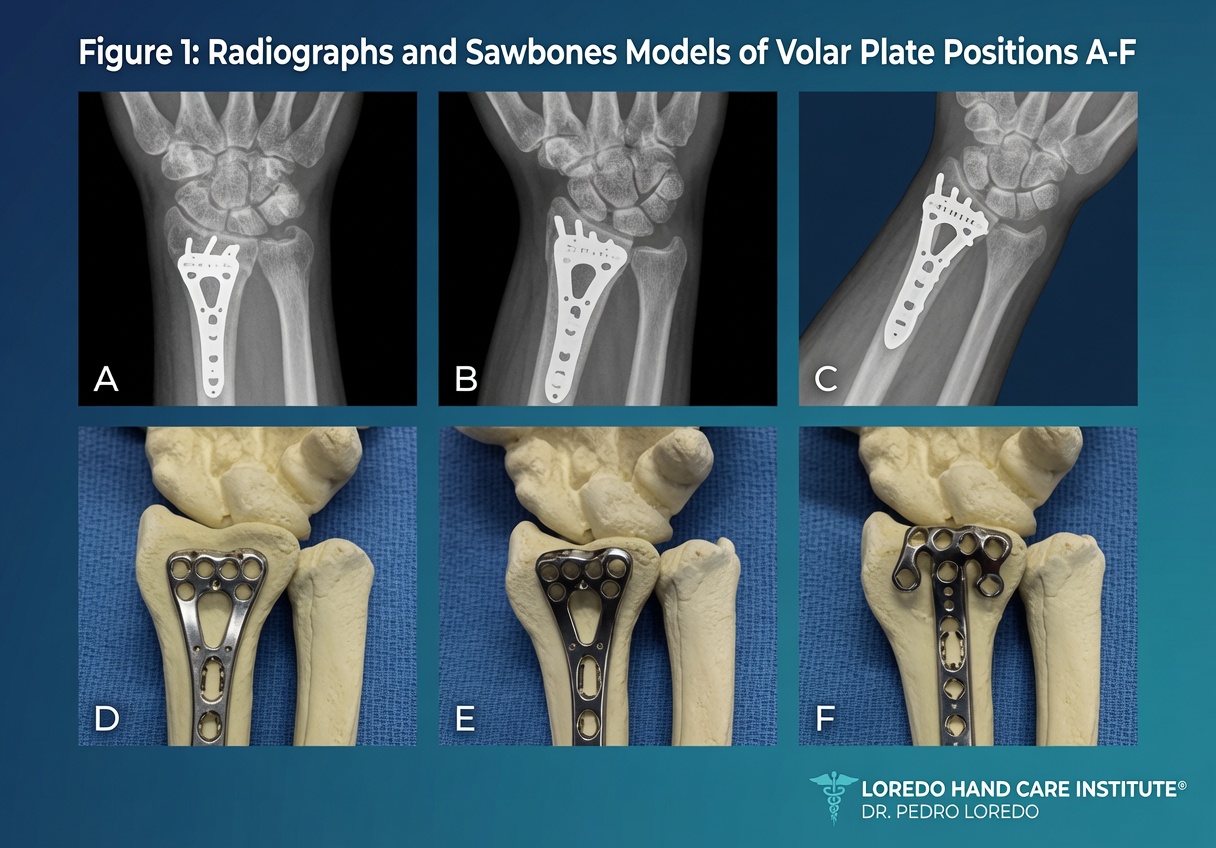
The workhorse for displaced unstable fractures. The fracture is exposed through a small surgical incision, reduced under direct view, and held with low-profile plates and screws. The volar locking plate has revolutionized distal radius fracture treatment because it provides stable fixation that allows protected motion within 1 to 2 weeks. Mini-plates and headless screws are used for metacarpal and phalanx fractures. Allows the fastest return to function for most fracture patterns.
Percutaneous Scaphoid Screw Fixation
A specialized technique for scaphoid fractures. A single compression screw is placed through a small skin puncture along the long axis of the scaphoid, providing stable internal fixation through a minimally invasive approach. Often preferred for proximal pole fractures (which have poor healing biology) and for displaced waist fractures. Allows earlier return to activity than cast immobilization alone.
External Fixation
An external frame holds bone fragments in alignment using pins that pass through the skin into the bone, connected to bars outside the body. Used for severely comminuted distal radius fractures, open fractures with extensive soft-tissue damage, and certain pediatric injuries. Often a temporary measure followed by definitive ORIF in a second stage.

Anesthesia Options
- Local anesthesia or hematoma block: for closed reduction in the office or emergency department.
- Regional axillary or supraclavicular block: for percutaneous pinning, ORIF, and percutaneous scaphoid screw. The arm is numbed for several hours.
- General anesthesia: for complex multi-fracture patterns, open fractures with extensive soft-tissue work, and patient preference.
Procedure Duration and Setting
- Closed reduction with cast: 30 to 45 minutes in office or ED.
- Percutaneous pinning: 30 to 60 minutes at an ASC, same-day discharge.
- Distal radius ORIF (volar plate): 60 to 90 minutes at an ASC, same-day discharge.
- Phalanx or metacarpal ORIF: 30 to 75 minutes at an ASC, same-day discharge.
- Percutaneous scaphoid screw: 30 to 60 minutes at an ASC, same-day discharge.
- External fixation for severe injuries: typically performed in the hospital, may include inpatient stay.
Recovery Timeline
- Phalanx and metacarpal fractures: cast or splint 3 to 4 weeks, hand therapy starting at week 2 to 3, full strength at 8 to 12 weeks.
- Distal radius volar plate ORIF: short arm splint 1 to 2 weeks, then progressive motion. Hand therapy starts at 1 to 2 weeks. Bone healing 6 to 8 weeks. Full strength at 12 to 16 weeks.
- Distal radius cast treatment: short arm cast 4 to 6 weeks, then hand therapy. Full strength at 12 to 16 weeks.
- Scaphoid percutaneous screw: short arm thumb spica splint 2 to 4 weeks, then progressive activity. Bone healing 8 to 12 weeks. Full strength at 16 weeks.
- Scaphoid cast treatment: long arm thumb spica cast 6 weeks then short arm thumb spica cast 6 weeks. Full strength at 16 to 20 weeks.
- External fixation followed by ORIF: variable; typically 12 to 16 weeks total recovery.
Return to Work and Daily Activities
- Office or desk work in a cast or splint: within days to a week
- Light manual labor: 4 to 8 weeks depending on bone and fixation
- Heavy manual labor: 8 to 16 weeks
- Driving: when out of cast or splint and able to grip the wheel safely; 2 to 6 weeks for most patients
- Contact sports and weightlifting: 3 to 6 months depending on fracture pattern
Why the Right Method Matters
- Anatomic restoration: intra-articular fractures heal better with surgical fixation that restores the joint surface to within 1 mm of normal.
- Stable fixation allows early motion: volar plate fixation of the distal radius allows protected motion within 1 to 2 weeks, dramatically reducing stiffness compared to 6 weeks of cast immobilization.
- Scaphoid fixation prevents nonunion: percutaneous screw fixation accelerates healing and reduces the risk of nonunion that can lead to wrist arthritis years later.
- Rotational correction: a malrotated metacarpal or phalanx will produce finger overlap when the patient makes a fist; surgical fixation corrects rotation that cast treatment cannot.
- Faster return to work: ORIF often shortens the time to return to work by weeks compared to cast treatment alone.
Risks and Complications
- Nonunion or malunion: the fracture fails to heal or heals in a poor position. Most often associated with scaphoid waist fractures, severe comminution, or noncompliance with immobilization.
- Stiffness: the most common long-term issue; minimized with early protected motion and consistent hand therapy.
- Hardware-related symptoms: tendon irritation or sensitivity over a plate may require hardware removal at 6 to 12 months after healing.
- Pin-tract infection: superficial infection at the entry site of K-wires; treated with local care and antibiotics.
- Tendon rupture: rare; the EPL tendon is the recognized late risk after distal radius fracture.
- Acute carpal tunnel syndrome after distal radius fracture from swelling and displacement; may require emergency carpal tunnel release.
- Complex regional pain syndrome (CRPS): rare but recognized after any wrist or hand fracture.
- Nerve injury from surgical exposure or pin placement; rare with careful technique.
- Standard surgical risks: bleeding, infection, anesthesia-related complications.
Cost and Insurance
Hand fracture fixation procedures are covered by virtually all commercial insurance plans, Medicare, the VA Community Care Network, and Texas workers' compensation when the fracture is documented and the procedure is medically indicated. Acute fractures are evaluated and treated as urgent regardless of insurance status; financial counseling occurs after definitive care. Our team verifies your benefits before any planned surgery. Call our office at (972) 939-4974 for a benefits check.
Frequently Asked Questions
How is the right fixation method chosen?
Method matched to fracture pattern. Stable nondisplaced fractures are treated with cast or splint immobilization alone. Displaced but easily reducible fractures may be treated with closed reduction and percutaneous pinning (K-wires). Comminuted, intra-articular, or unstable fractures usually need open reduction with internal fixation (ORIF) using plates and screws. Severely contaminated or open fractures with extensive soft-tissue damage often start with external fixation followed by definitive fixation in a second stage. The choice depends on the bone, the fracture pattern, the displacement, the patient's hand demands, and the soft-tissue condition.
Why is a scaphoid fracture different?
The scaphoid bone has a unique blood supply that enters at the distal end and runs back through the bone in a retrograde direction. A fracture across the middle (waist) of the scaphoid can cut off blood supply to the proximal half. Without prompt and correct treatment, the proximal scaphoid can fail to heal (nonunion) or die (avascular necrosis). For this reason, displaced scaphoid fractures are often treated with percutaneous screw fixation rather than cast alone, even when the displacement is minimal. The screw provides compression across the fracture site, accelerates healing, and shortens the recovery time. Proximal pole scaphoid fractures are particularly likely to need surgical fixation.
How long am I in a cast or splint?
Variable by bone and fixation method. Phalanx and metacarpal fractures treated with closed methods are typically immobilized 3 to 4 weeks. Distal radius fractures are immobilized 4 to 6 weeks (less if internally fixed with a volar plate that allows protected motion within 1 to 2 weeks). Scaphoid fractures are immobilized 6 to 12 weeks depending on location and fixation. Hand therapy starts as soon as the fracture is stable enough to allow protected motion.
Will I be able to use my hand normally again?
Most patients with stable closed fractures recover near-normal hand function with appropriate treatment and structured hand therapy. Functional outcomes after distal radius volar plate fixation are excellent. Stiffness is the most common long-term issue and is minimized with early protected motion and consistent hand therapy. Complex intra-articular fractures, scaphoid nonunion, and fractures with associated tendon or nerve injury have somewhat lower functional ceilings, but most patients return to their pre-injury occupation and recreational activity.
What if my fracture has already started healing in a bad position?
Malunion (a fracture that healed in a poor position) and nonunion (a fracture that did not heal) can be treated with corrective osteotomy and revision fixation. The procedure realigns the bone and fixes it in correct anatomic position, often with bone grafting to support healing. Outcomes are good when the right indication exists, but the procedure is more complex than primary fixation. Coming to a hand surgeon promptly after injury is the best way to avoid these complications.
Related Conditions
- Hand and Finger Fractures: the underlying conditions this procedure treats. Distal radius, scaphoid, boxer's, and phalanx fractures.
- TFCC Tears: a TFCC tear coexists with up to 50 percent of distal radius fractures and may be addressed at the time of fracture fixation.
- Carpal Tunnel Syndrome: acute carpal tunnel syndrome can develop after distal radius fracture; emergent carpal tunnel release is occasionally combined with fracture fixation.
- Hand and Wrist Arthritis: post-traumatic arthritis is a long-term consequence of poorly healed or untreated fractures.
- Workers' Compensation Injuries: workplace fractures treated under Texas WC.
Related Procedures
- Microsurgery: combined with fracture fixation in open injuries with associated nerve or vessel laceration.
- Endoscopic Carpal Tunnel Release: occasionally performed at the time of distal radius fixation for acute carpal tunnel syndrome.
- All Procedures: the full list of surgical procedures offered at the practice.
From the Blog
- Distal Radius Fractures: Should You Get Surgery?: cast versus volar locking plate.
- Scaphoid Fractures: Why They Are Dangerous: retrograde blood supply and percutaneous screw fixation.
- Hand Therapy After Surgery: post-fracture motion progression.
Watch: Hand fracture fixation education
Short videos from Dr. Loredo's Instagram channel.