Workers' compensation hand and upper extremity injuries include lacerations, fractures, crush injuries, burns, and cumulative trauma disorders that result from work activity. In Texas, the workers' compensation system covers medical care, lost wages, and impairment benefits for injured workers whose employers carry workers' compensation insurance. Loredo Hand Care Institute treats workplace upper extremity injuries, coordinates directly with case managers and adjusters, provides MMI determinations and impairment ratings, and works with employers on appropriate return-to-work timing. There is no out-of-pocket cost to the injured worker for covered care.
Common Workplace Upper Extremity Injuries
The practice treats the full range of workplace hand, wrist, elbow, and forearm injuries.
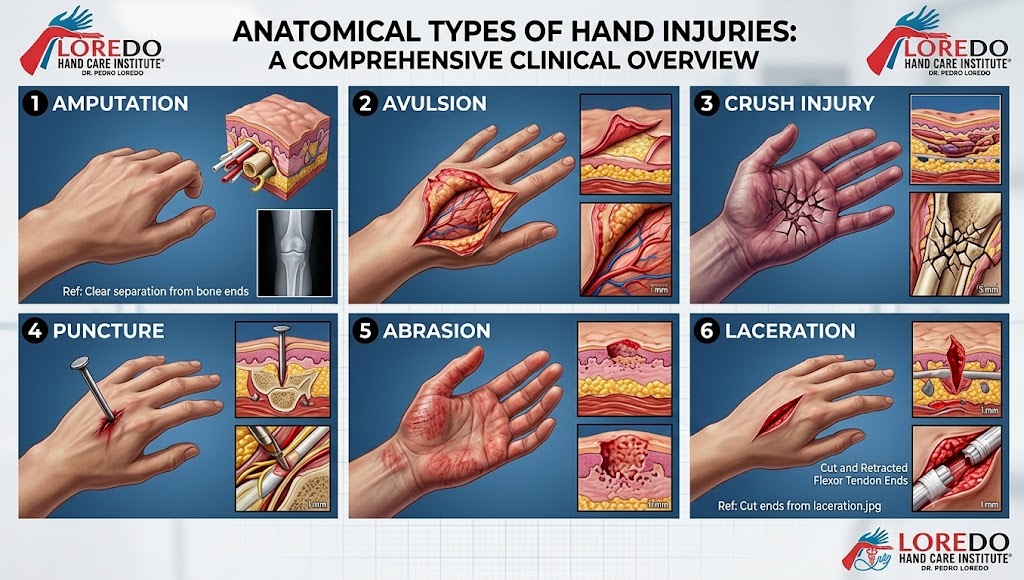
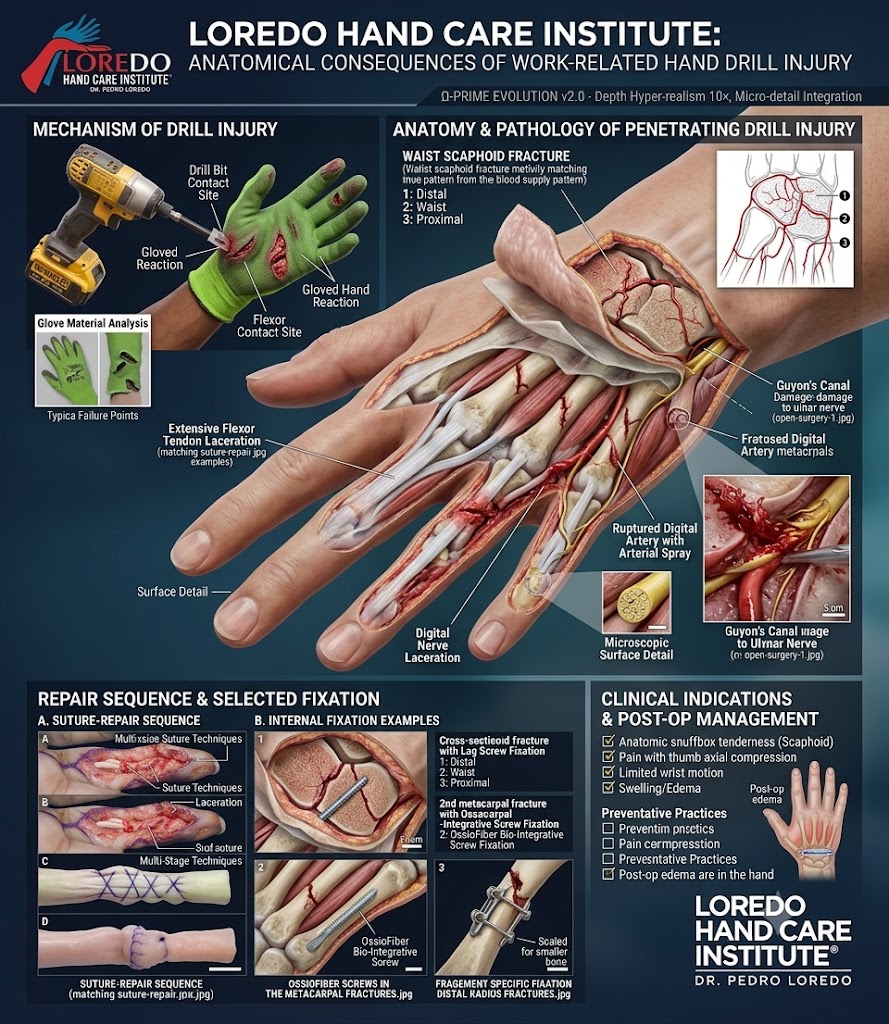
- Lacerations from blades, glass, sheet metal, broken bottles, and saws, with or without associated tendon, nerve, or vascular injury
- Fractures of the distal radius, scaphoid, metacarpals, and phalanges from falls, impact, and crush
- Crush injuries from rollers, presses, dropped loads, and rotating equipment
- Tendon injuries: flexor and extensor tendon lacerations, tendon avulsions, and ruptures
- Cumulative trauma disorders: carpal tunnel syndrome, cubital tunnel syndrome, trigger finger, lateral and medial epicondylitis, and De Quervain's tendonitis from repetitive work activity
- Burns and chemical injuries when hand surgery and reconstruction are needed
- Animal and human bites in the workplace, including infection management and any associated tendon injury
- Amputation injuries, including replantation when feasible and revision amputation when not
- Frostbite and cold injury in outdoor occupations during winter months
- Compartment syndrome, a surgical emergency from severe crush or constrictive injury

How Texas Workers' Compensation Works
Texas is unique in that workers' compensation coverage is optional for employers. Most large and mid-size employers carry traditional WC insurance through a private carrier. Some carry alternative non-subscriber plans that mimic WC benefits but are administered differently. A small number of employers carry no coverage at all, in which case workplace injuries fall outside the WC system and must be addressed through other channels.

For traditional WC injuries:
- The employer's insurance carrier (or its third-party administrator) is the payer
- The injured worker reports the injury to the employer and a claim is opened
- The injured worker selects a treating doctor from the carrier's network or list
- Authorization is obtained for evaluations, imaging, surgery, and therapy
- The treating doctor documents work status (off work, restricted duty, full duty) at each visit
- When the condition stabilizes, MMI is declared and an impairment rating is assigned
- The case proceeds to administrative closure with any indemnity benefits paid per Texas statute
The injured worker is not responsible for medical bills for covered treatment. There is no copay, deductible, or balance billing for authorized WC care.
How We Handle Your Case
Loredo Hand Care Institute manages workers' compensation cases as a structured pathway from injury to return to work to MMI.

- Pre-visit verification: our team verifies coverage with the carrier, obtains authorization for the evaluation, and confirms the date-of-injury (DOI) details before the appointment.
- Initial evaluation: Dr. Loredo performs a focused history and examination, orders any needed imaging, and establishes a working diagnosis. A treatment plan is documented and submitted to the carrier for authorization.
- Authorized treatment: conservative care, surgery, hand therapy, and any medications are coordinated with the carrier. Treatment progresses through the same evidence-based pathways used for non-WC patients.
- Work status documentation: at each visit, work status is documented and a copy is provided to the patient, the employer, and the carrier. Work status may be off work, restricted (with specific limitations on lifting, gripping, repetitive motion, or exposure), or full duty.
- Return-to-work coordination: when the patient is ready for restricted duty, our team works with the employer's HR or occupational health to identify appropriate light-duty positions. Restricted duty often shortens the overall recovery and reduces the risk of deconditioning.
- MMI and impairment rating: when the injury has stabilized and continued treatment would not produce further measurable improvement, MMI is declared. An impairment rating is assigned per the AMA Guides to the Evaluation of Permanent Impairment and submitted to the carrier.
Maximum Medical Improvement (MMI)
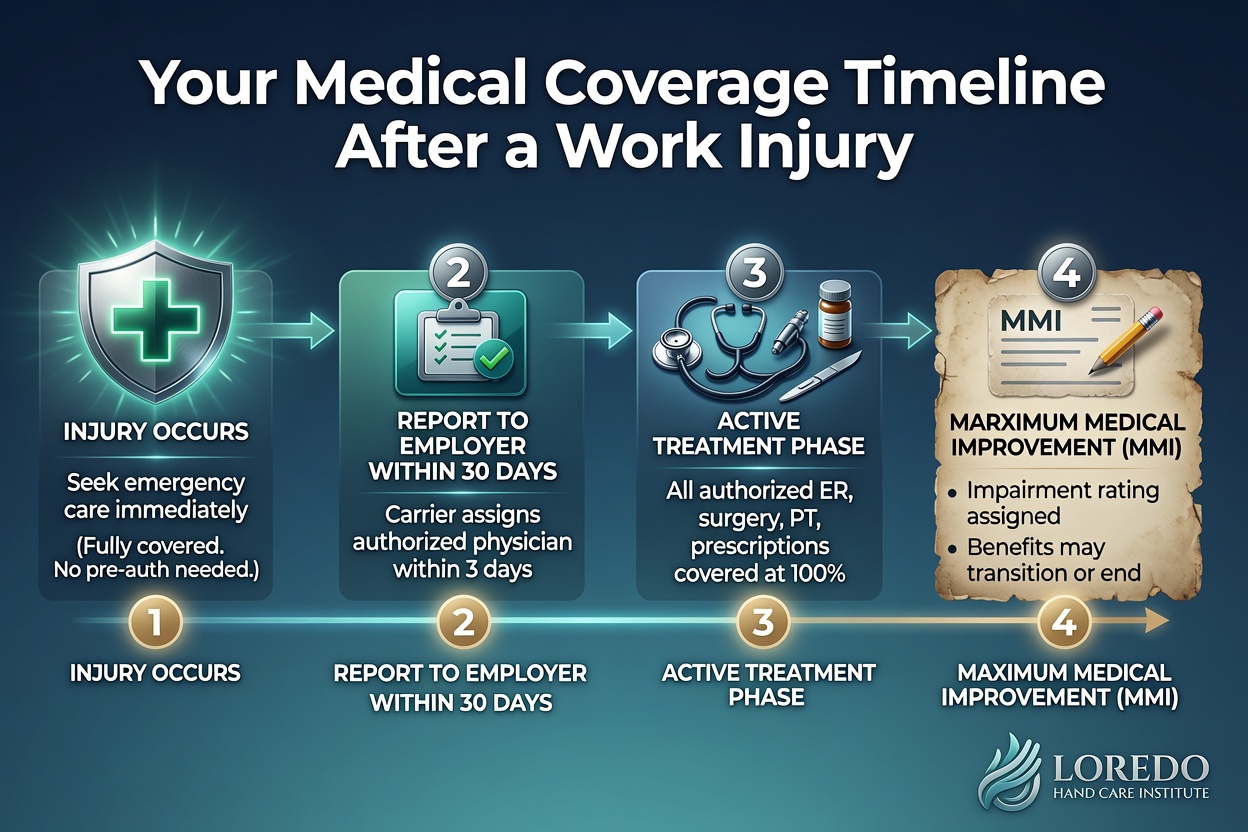
MMI is the point at which the work-related injury has stabilized and further medical treatment is not expected to substantially improve the condition. In Texas, MMI must be reached by 104 weeks from the date of injury unless an extension is granted. The treating physician determines MMI based on the trajectory of recovery, the response to surgery and therapy, and clinical judgment that further care will not produce measurable improvement.
MMI does not mean the patient is completely back to normal. It means the residual condition is what it is going to be. Some patients reach MMI with full function and no measurable impairment. Others reach MMI with permanent partial impairment that is captured in the impairment rating.
Impairment Ratings
An impairment rating quantifies the permanent loss of function from the work-related injury. The rating is calculated using the AMA Guides to the Evaluation of Permanent Impairment, which is the standard reference for Texas WC. The Guides translate measured findings (range of motion, sensory testing, strength, joint stability, amputation level) into percentages of whole-person impairment.
For hand injuries, common findings that contribute to an impairment rating include:
- Loss of motion at one or more joints
- Sensory loss in the median, ulnar, or radial nerve distributions
- Motor weakness or muscle atrophy
- Joint instability
- Amputation, with rating that depends on the level
- Pain documented per the relevant chapter of the Guides

The impairment rating is a medical determination, not a financial one. The Texas Department of Insurance Division of Workers' Compensation translates the rating into indemnity benefits per statute.
Functional Capacity Evaluation (FCE)
An FCE is a structured set of physical performance tests, typically performed by a hand therapist or occupational therapist over 2 to 4 hours, that documents the worker's current capacity for lifting, gripping, manipulation, and sustained activity. FCEs are ordered when the work demands are heavy, when restricted duty options are limited, when the employer needs documented capacity to make accommodation decisions, or when there is a question about whether the worker can return to the same job. Dr. Loredo orders an FCE through a credentialed hand therapy partner when one is appropriate for the case.

Communicating with Adjusters and Case Managers
The case manager or adjuster is the carrier's representative who coordinates authorization, payment, and case progression. Effective communication shortens the recovery and avoids administrative delay.
- Authorization is obtained in advance for all evaluations, imaging, surgery, therapy, and durable medical equipment. Our office submits the requests with appropriate clinical documentation.
- Case manager updates are provided after each visit with a summary of clinical findings, work status, and next steps.
- Phone calls and conferences are accommodated when the case manager has specific questions about diagnosis, treatment plan, expected timeline, or return-to-work options.
- Required forms (DWC-73 work status reports, DWC-69 MMI/impairment rating, and equivalent forms for non-subscriber plans) are completed and submitted within statutory deadlines.
- Peer-to-peer consultations with the carrier's medical director are conducted when authorization is delayed or denied for medically necessary care.
Return to Work
Return to work is staged to match the trajectory of recovery and the demands of the job.
- Off work: reserved for the immediate post-operative period, severe acute injuries, and conditions that require complete rest. Typically 1 to 4 weeks for most upper extremity surgeries.
- Restricted duty: the most common phase. Specific limitations are documented (no lifting over X pounds, no repetitive gripping, no power tool use, no exposure to wet or sharp environments, dominant or non-dominant hand restricted, splint or brace in place). Restricted duty maintains conditioning and reduces the risk of prolonged disability.
- Full duty: declared when the worker has completed appropriate recovery and demonstrated the capacity to perform all essential job functions safely.
Coordination with the employer's HR and occupational health team is the most important factor in successful return to work. Employers who can offer meaningful restricted duty typically see shorter total disability periods and better long-term outcomes for their workers.
Frequently Asked Questions
Does Loredo Hand Care Institute accept workers' compensation patients?
Yes. The practice accepts Texas workers' compensation patients for hand, wrist, elbow, and upper extremity injuries. Our team verifies coverage with the carrier before the first visit, communicates directly with the adjuster and case manager, and submits all required documentation. There is no out-of-pocket cost to the injured worker for covered care. We also accept the federal subscriber options that some Texas employers carry instead of traditional WC.
What injuries are commonly covered under workers' compensation?
The most common workplace upper extremity injuries we treat are hand and finger lacerations from blades, glass, or sheet metal; fractures of the distal radius, scaphoid, metacarpals, and phalanges; crush injuries from rollers, presses, or dropped loads; cumulative trauma disorders including carpal tunnel and trigger finger; and tendon injuries from machinery contact. Animal and human bites in the workplace are also covered when work-related.
What does MMI mean and when is it determined?
Maximum medical improvement (MMI) is the point at which a work-related injury has stabilized and further medical treatment is not expected to substantially improve the condition. In Texas, MMI must be reached by the statutory deadline (104 weeks from the date of injury) unless an extension is granted. Once MMI is reached, a designated examining physician assigns an impairment rating based on the AMA Guides, and the case proceeds to closure. We document MMI when the patient has completed appropriate surgery, hand therapy, and return-to-work coordination, and when continuing the same plan would not produce further measurable improvement.
Will my employer find out about my injury?
Workers' compensation is by design a system that involves the employer in covering work-related care. The employer's WC carrier or third-party administrator is the payer, and the case manager or adjuster coordinates authorization. Specific medical details beyond what is necessary for return-to-work decisions are protected by HIPAA and are not shared with the employer's HR or management. Our office handles all WC paperwork directly with the carrier and only releases information that the patient has authorized.
How quickly can I be seen after a workplace injury?
Most workers' compensation hand injuries are seen the same day or next day. Acute injuries (lacerations, fractures, fresh crush injuries) are treated as urgent. Cumulative trauma evaluations (carpal tunnel, trigger finger, lateral epicondylitis) are typically scheduled within a week of authorization. Surgical procedures, when indicated, are scheduled promptly to keep the patient on the path to maximum medical improvement and timely return to work.
When to Call
Call our office for any of the following workplace upper extremity issues:
- A laceration, fracture, crush, or other acute injury that occurred at work
- Persistent hand, wrist, or elbow symptoms that you believe are work-related (cumulative trauma)
- A workers' compensation claim that has been opened and needs an authorized treating physician
- A second opinion request from a case manager or adjuster
- An MMI evaluation or impairment rating request
- Coordination of return-to-work after a previous WC injury
Open lacerations with active bleeding, severe crush injuries, finger amputations, deformities with skin compromise, and signs of compartment syndrome are emergencies. Call 911 or go to the nearest emergency department immediately, then call our office to coordinate follow-up WC care.
Related Conditions
- Hand and Finger Fractures: distal radius, scaphoid, boxer's, and phalanx fractures, all common workplace injuries.
- Flexor Tendon Injury: lacerations of the flexor tendons from blades, glass, or sheet metal, requiring prompt repair.
- Extensor Tendon Injury: dorsal hand and finger lacerations, including mallet finger from jamming injuries on the job.
- Carpal Tunnel Syndrome: the most common cumulative trauma disorder claimed under WC for upper extremity.
- Trigger Finger: another cumulative trauma claim, particularly in workers with repetitive forceful gripping.
- Cubital Tunnel Syndrome: ulnar nerve compression at the elbow in workers with prolonged elbow flexion or direct pressure on the elbow.
- Tennis Elbow: lateral epicondylitis from repetitive forceful gripping in manual occupations.
- Veterans Care: similar coordination with VA Community Care Network for veteran patients.
From the Blog
- Returning to Work After Hand Surgery: timelines, FMLA paperwork, and work restrictions.
- Ergonomic Tips for Hand Pain: workplace strategies to prevent re-injury.
Watch: Workplace hand injury education
Short videos from Dr. Loredo's Instagram and Facebook channels.