Hand and wrist masses are common, and the great majority are benign. Ganglion cysts alone account for 60 to 70 percent of all hand masses. Other common benign lesions include lipomas, epidermal inclusion cysts, giant cell tumors of the tendon sheath, schwannomas, glomus tumors, and mucous cysts. Malignant tumors of the hand are rare. The most important step in evaluation is accurate diagnosis: distinguishing the typical benign pattern (slow-growing, painless, mobile, classic location) from the red flags that warrant prompt biopsy (rapid growth, deep fixation, pain at rest, history of cancer, ulceration). Treatment ranges from observation of asymptomatic benign masses to needle aspiration, surgical excision, and oncologic referral when malignancy is suspected.
Common Benign Hand Masses
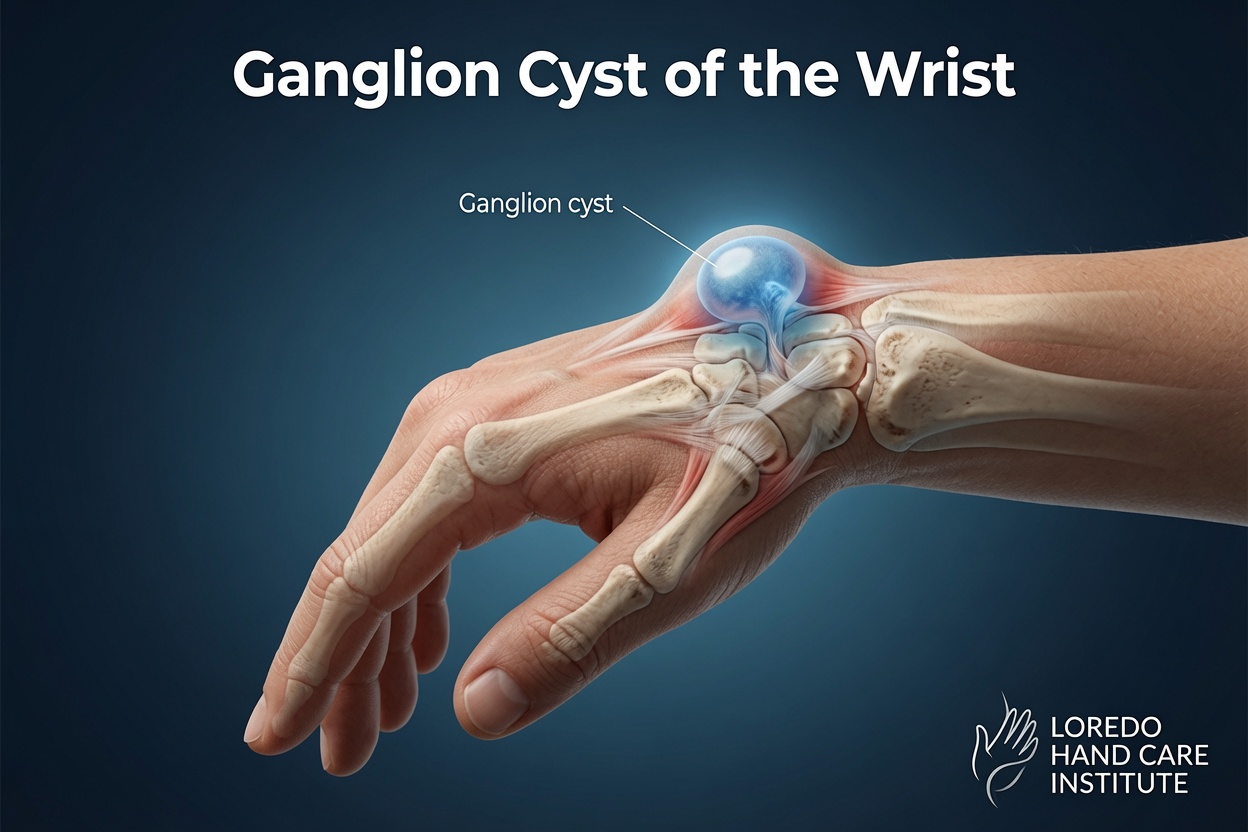
Ganglion Cysts
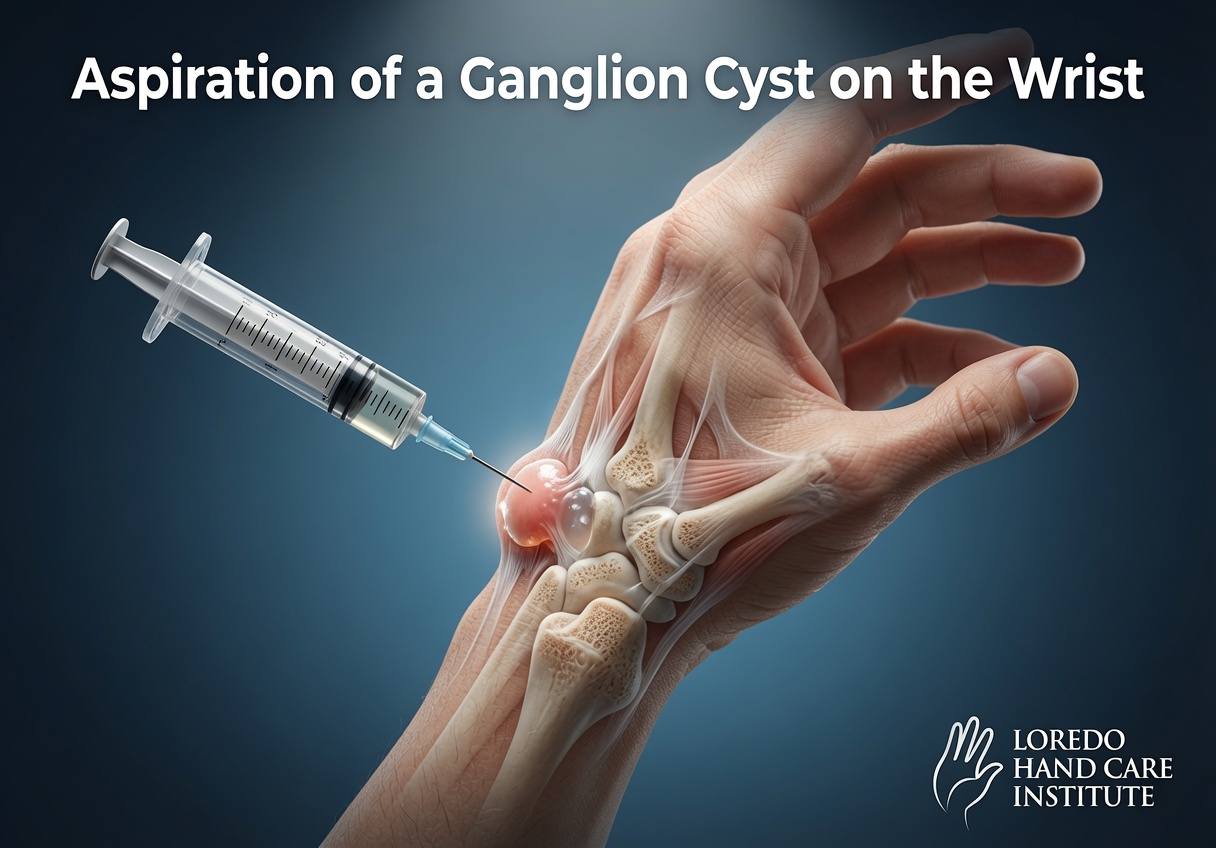
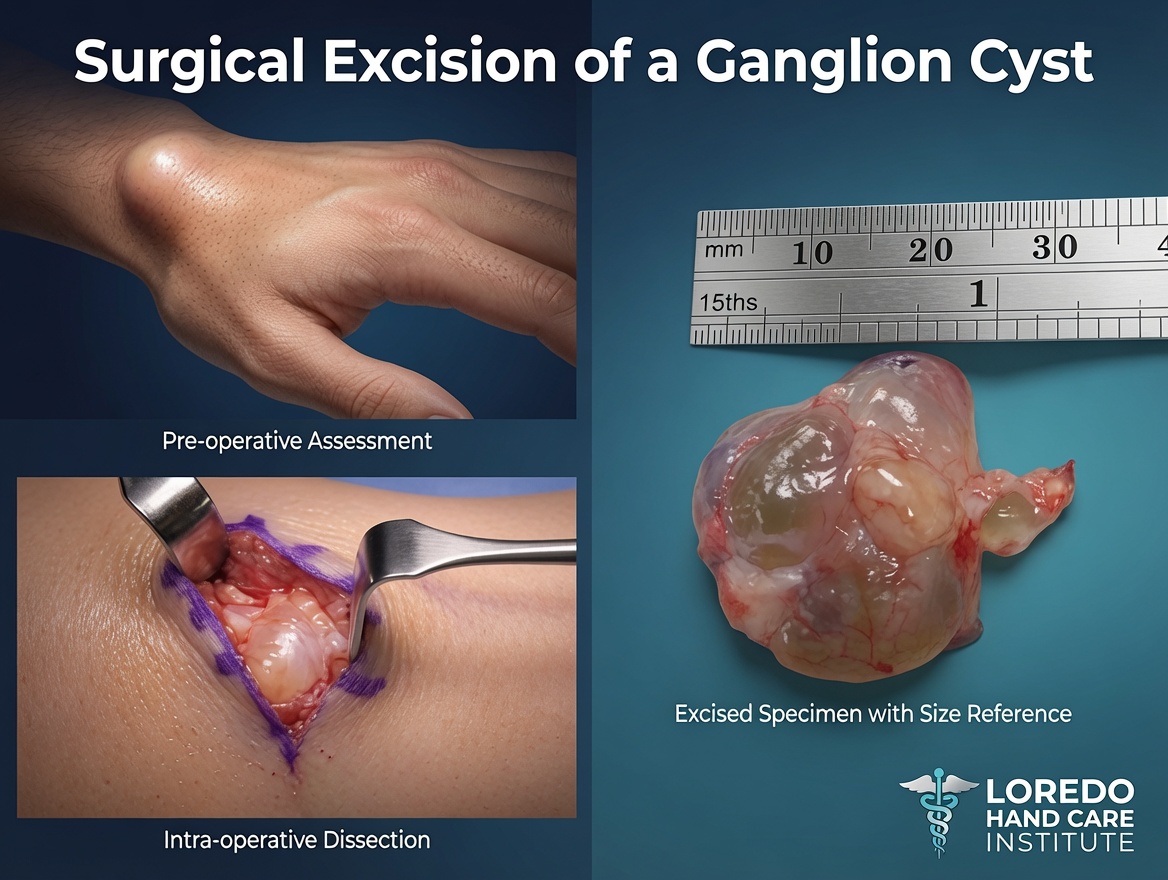
Fluid-filled cysts that arise from a joint capsule or tendon sheath. The most common location is the dorsal wrist (over the scapholunate ligament), followed by the volar wrist (over the radioscaphoid joint), and the volar finger (retinacular ganglion at the A1 pulley). Ganglion cysts fluctuate in size, often increase with activity, and may transilluminate (a flashlight pressed against the cyst lights it up because of the fluid content). Treatment options include observation, needle aspiration, and surgical excision. Many ganglion cysts spontaneously resolve over months.
Epidermal Inclusion Cysts
Slowly enlarging round cysts that arise after a small puncture wound implants a fragment of skin into the deeper tissue. The implanted skin continues to produce keratin, which accumulates and forms the cyst. Common locations include the palm, finger pulp, and beneath fingernails. Treatment is surgical excision when symptomatic.
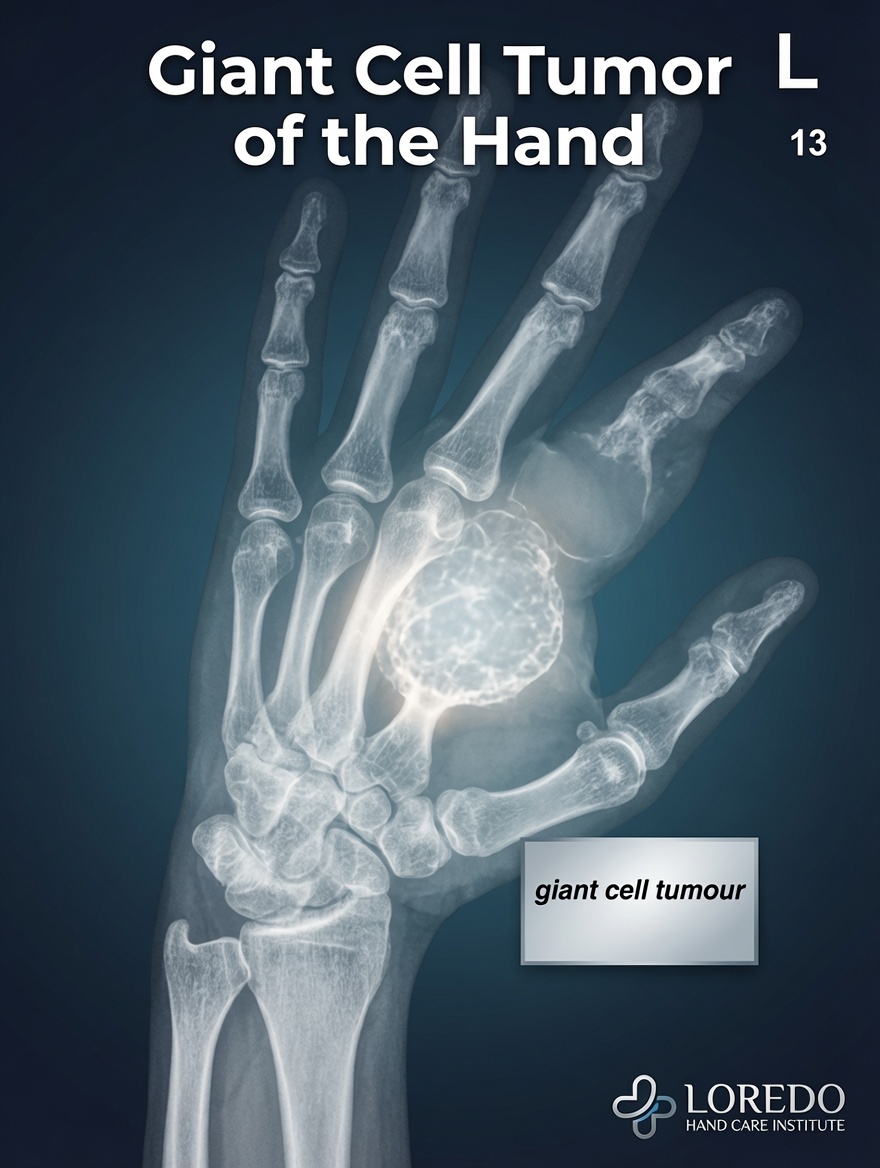
Giant Cell Tumor of the Tendon Sheath
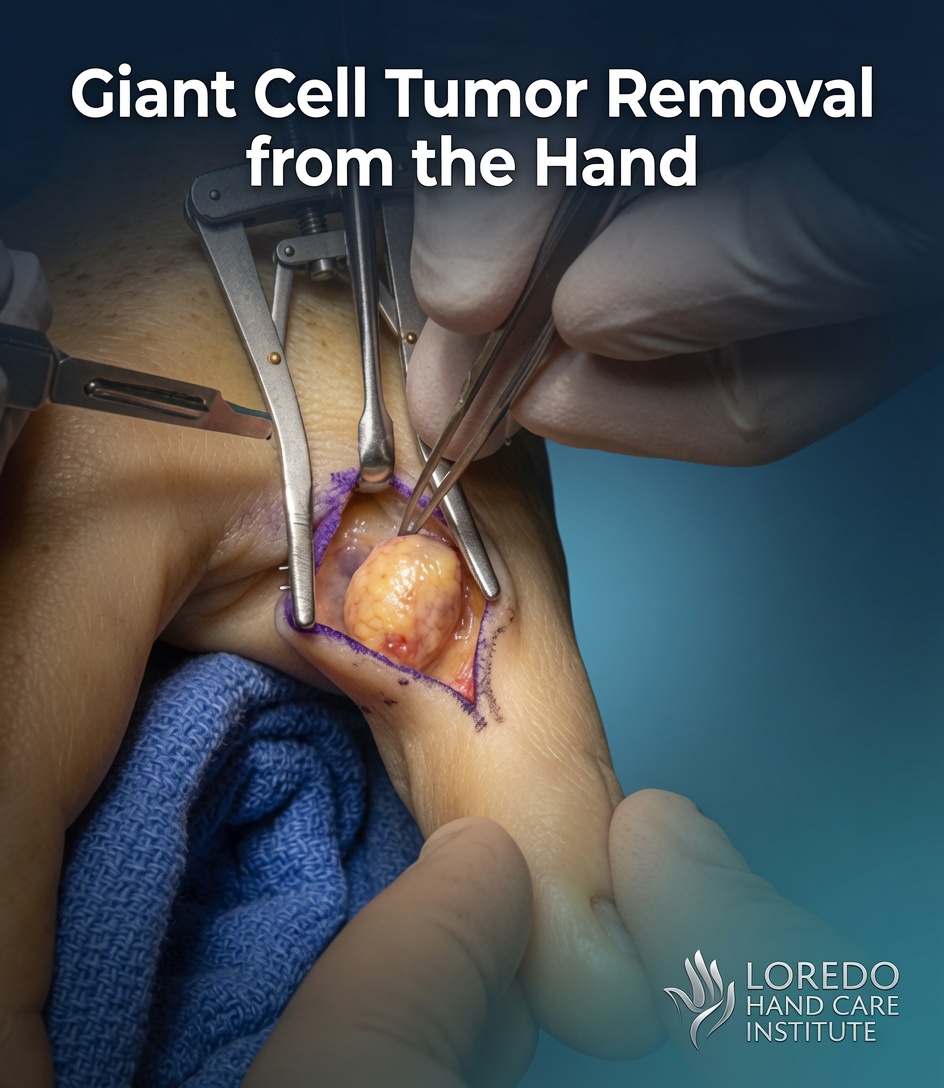
The second most common solid mass of the hand. Arises from the synovial lining of a tendon sheath, most often on the volar (palm) side of a finger. Firm, slow-growing, and usually painless. Surgical excision is the treatment of choice. Recurrence after excision is approximately 10 to 15 percent.
Lipomas
Benign tumors of mature fat. Soft, mobile, and slow-growing. Most lipomas of the hand are small and asymptomatic, but larger lipomas can produce pressure on nerves or restrict tendon gliding. Excision is straightforward when symptoms warrant it.
Schwannomas (Nerve Sheath Tumors)
Benign tumors that arise from the Schwann cells surrounding peripheral nerves. Small schwannomas may be asymptomatic, but larger ones can produce a Tinel sign (electric tingling in the nerve distribution when tapped) and sometimes weakness. Excision is performed under microscope to preserve the underlying nerve fascicles.
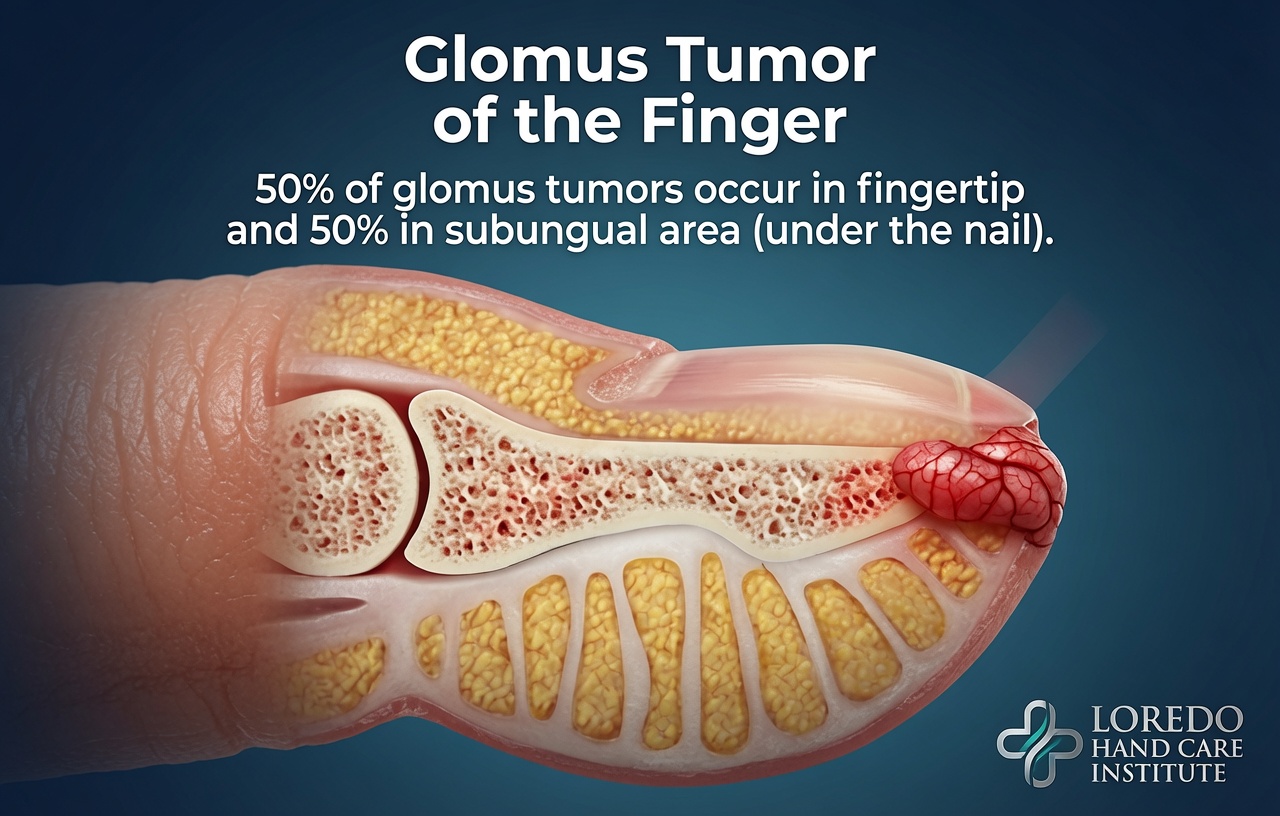
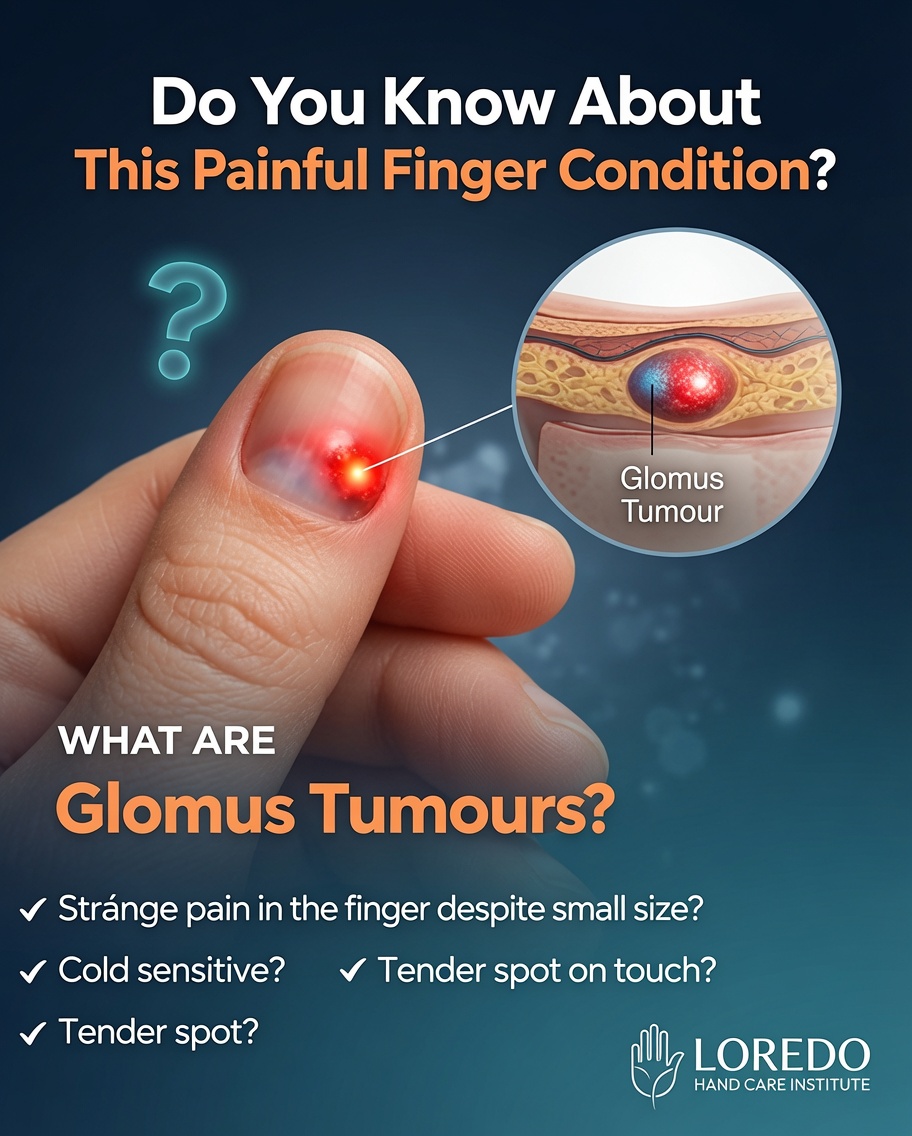
Glomus Tumors
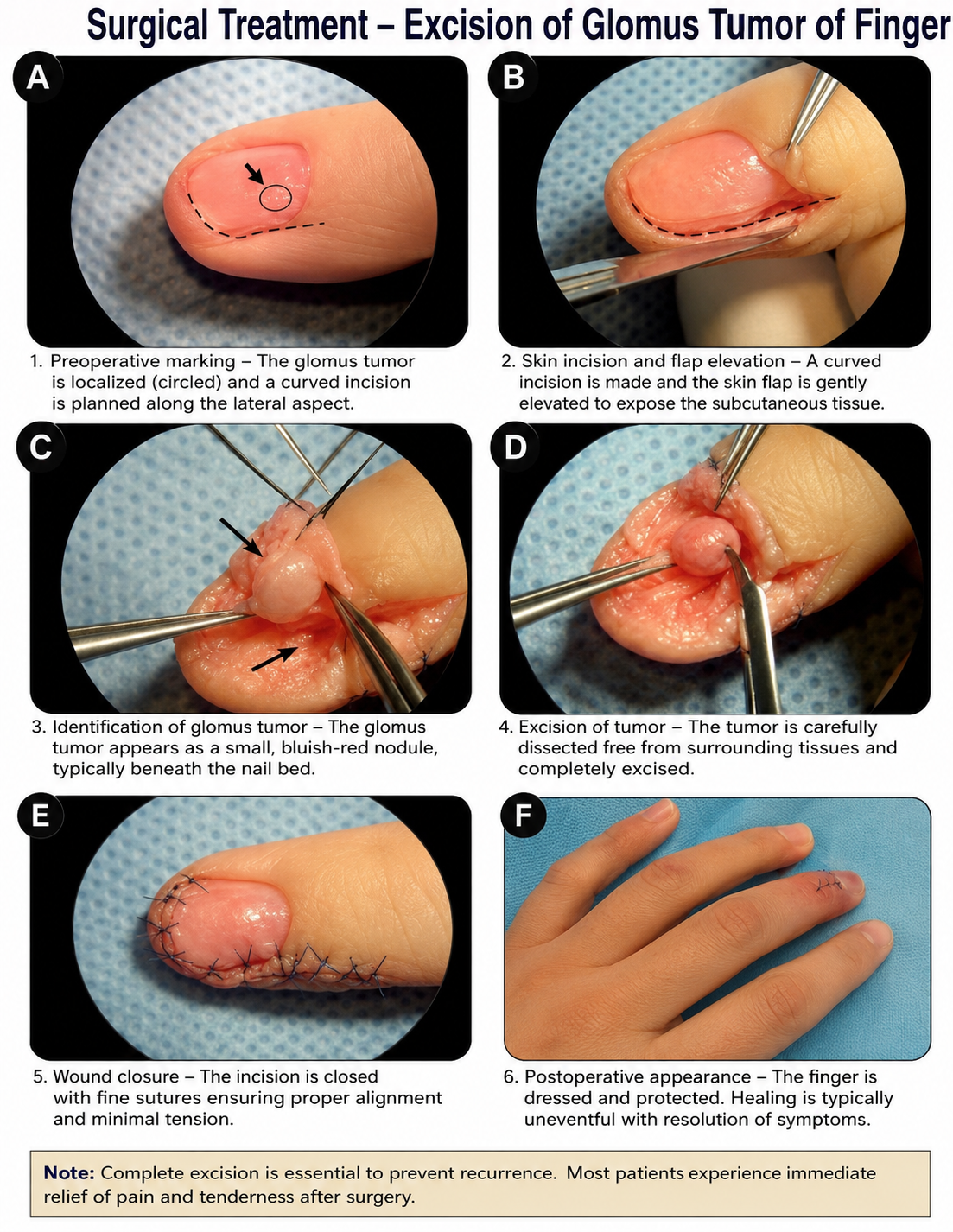
Small benign tumors of the temperature-regulating glomus body, most often located beneath a fingernail. The classic clinical triad is severe localized pain, exquisite cold sensitivity, and point tenderness with a paperclip pressed against a specific spot under the nail. A bluish discoloration may be visible through the nail. MRI confirms the diagnosis. Surgical excision through a transungual or lateral approach is curative.
Mucous Cysts
Specific subtype of ganglion cyst that arises from the DIP joint, almost always associated with underlying osteoarthritis. Located on the dorsum of the fingertip near the cuticle. May produce nail deformity from pressure on the nail matrix. Treatment is surgical excision combined with osteophyte removal at the underlying DIP joint.
Post-Traumatic Neuromas
Disorganized regenerating nerve tissue that forms after a nerve has been cut, crushed, or injured. Produces a tender bump with electric tingling when tapped. Surgical revision (excision or relocation of the nerve end) is performed when the neuroma is painful and limiting.
Clinical coding: ICD-10 D21.10 (benign neoplasm of soft tissue, upper limb), D17.20 (lipoma upper limb), D36.7 (other benign neoplasm). SNOMED CT 41003003 (mass of upper extremity).
Red Flags That Warrant Prompt Evaluation
Most hand masses are benign, but certain features warrant urgent attention:
- Rapid growth over weeks rather than months or years
- Hard, fixed mass that does not move with the underlying tissue
- Pain at rest, not just with motion or pressure
- Ulceration or skin breakdown overlying the mass
- Personal history of cancer, particularly breast, lung, or melanoma
- Unexplained weight loss or other systemic symptoms
- Mass larger than 5 cm
- Associated nerve symptoms (constant numbness, weakness, or muscle wasting)
- Pulsatile mass (suggests vascular tumor or aneurysm)
- Mass located deep in the muscle compartment rather than just under the skin
The threshold for evaluation is intentionally low. The cost of a workup is small. The cost of a missed malignancy is high.
How the Diagnosis Is Made
Most hand masses can be diagnosed clinically with high confidence based on location, character, and history. Imaging and biopsy are used selectively.
- Physical examination: location, size, mobility, fluctuance, tenderness, transillumination, Tinel sign, skin changes.
- Transillumination test: a flashlight pressed against a fluid-filled mass like a ganglion cyst illuminates the cyst, distinguishing it from solid tumors.
- Plain radiographs: rule out underlying bony abnormality, calcifications, or pressure erosion of bone (suggests a longer-standing or more aggressive lesion).
- Ultrasound: the first-line imaging for most hand masses. Distinguishes solid from cystic lesions, evaluates blood flow, and is fast, inexpensive, and free of radiation.
- MRI: the imaging of choice for deep, atypical, or potentially aggressive masses. Provides detailed anatomic information about the relationship to tendons, nerves, and bone.
- Needle biopsy or open biopsy: performed when imaging or clinical features raise concern for malignancy. The biopsy approach is planned to allow definitive surgical excision in the same incision if malignancy is confirmed.
Treatment Options
Observation
Asymptomatic benign masses with classic features can often be observed. Many ganglion cysts spontaneously resolve over months. Small lipomas, stable inclusion cysts, and asymptomatic schwannomas may need no intervention.
Aspiration
Needle aspiration of a ganglion cyst can be performed in the office under local anesthesia. The cyst contents (a thick gelatinous fluid) are withdrawn through a needle. Recurrence is common (50 to 70 percent over 1 to 2 years), but the procedure is fast, low-risk, and may avoid surgery. Inclusion cysts and giant cell tumors do not respond to aspiration.
Surgical Excision
Outpatient surgery under local or regional anesthesia. The mass is removed in its entirety, including the underlying connection to a joint capsule or tendon sheath when present (essential for ganglion cyst recurrence prevention). Microsurgical technique is used for nerve-related tumors to preserve the underlying nerve. Recovery is usually 2 to 6 weeks depending on the location.
Oncologic Referral
When biopsy confirms malignancy, the patient is referred to a sarcoma surgical oncologist or hand oncologist for definitive resection, often with adjuvant therapy. The approach changes substantially: wide margins, possible reconstruction, and coordination with medical and radiation oncology. Hand sarcomas are rare but require specialized management.
Recovery Timeline
- Aspiration: same-day return to most activity. Mild bruising. Recurrence may occur over weeks to months.
- Excision of small superficial mass: 1 to 2 weeks of dressing, return to office work within days, full activity within 2 to 3 weeks.
- Excision of larger or deeper mass: 2 to 4 weeks of dressing and protection, full activity within 4 to 6 weeks.
- Excision of nerve-related tumor (schwannoma): 4 to 6 weeks of recovery with hand therapy as needed; sensory recovery may continue over months.
- Excision of glomus tumor: 2 to 4 weeks for nail and skin healing; full activity within 4 weeks.
- Excision of mucous cyst with osteophyte removal: 4 to 6 weeks; sometimes a small splint is used.
Returning to Work and Daily Activity
- Office or desk work: within days for most procedures
- Light manual labor: 2 to 3 weeks for superficial excisions; 4 to 6 weeks for deeper or nerve-related excisions
- Heavy manual labor: 4 to 6 weeks for most cases; 8 to 12 weeks for sarcoma resection with reconstruction
- Driving: within days for office procedures; 1 to 2 weeks for surgical excision
Frequently Asked Questions
Are most hand masses cancerous?
No. The great majority of hand and wrist masses are benign. Ganglion cysts alone account for 60 to 70 percent of all hand masses. Other common benign masses include lipomas, epidermal inclusion cysts, giant cell tumors of the tendon sheath, schwannomas, and glomus tumors. Malignant tumors of the hand are rare. The most important step is accurate diagnosis: most benign masses can be observed or excised electively, while a small minority warrant prompt evaluation and possible biopsy. Red flags that suggest a more serious lesion include rapid growth, deep fixation, pain at rest, history of cancer elsewhere, ulceration of the overlying skin, and a history of unexplained weight loss.
Should I aspirate or excise my ganglion cyst?
Aspiration with a needle is a reasonable first step for symptomatic dorsal wrist or volar wrist ganglion cysts. The procedure can be done in the office and produces immediate decompression. Recurrence after aspiration is common, with reported rates of 50 to 70 percent. Surgical excision through a small incision has a recurrence rate of 5 to 15 percent and is the more durable option. The choice depends on the size, location, severity of symptoms, and whether the cyst has recurred after a prior aspiration. Asymptomatic ganglion cysts often need no treatment at all and frequently resolve spontaneously.
What is a glomus tumor and why does it hurt?
A glomus tumor is a small benign tumor of the temperature-regulating glomus body, which is concentrated under the fingernails. Glomus tumors are tiny (often only 2 to 5 mm) but produce disproportionate pain because of their innervation. The classic triad is point tenderness with a paperclip or pin pressed against a specific spot under the nail, severe cold sensitivity at that spot, and constant pain that worsens at night. A bluish or pink discoloration may be visible through the nail. MRI confirms the diagnosis. Excision through a transungual or lateral approach is curative.
What is a giant cell tumor of the tendon sheath?
Giant cell tumor of the tendon sheath (also called pigmented villonodular synovitis of the tendon sheath) is the second most common solid mass of the hand after ganglion cysts. It is a benign tumor that arises from the synovial lining of a tendon sheath, most often on the volar (palm side) of a finger. The mass is firm, slow-growing, and often painless. Surgical excision is the treatment of choice. Recurrence after excision is approximately 10 to 15 percent because the tumor can extend along the tendon sheath in subtle ways.
When should I worry about a hand mass?
Most hand masses are benign and not urgent. Red flags that warrant prompt evaluation include: rapid growth over weeks rather than months or years, a mass that is hard, fixed to underlying bone or tendon, pain at rest (not just with motion), ulceration or skin changes overlying the mass, a personal history of cancer (particularly breast, lung, or melanoma), unexplained weight loss, and a mass larger than 5 cm. Imaging (ultrasound first, MRI for atypical masses) and biopsy are appropriate when red flags are present. The threshold for evaluation is low because the consequence of missing a malignancy is high.
When to Call the Doctor
Call our office for evaluation if you experience:
- Any new hand or wrist lump that has been present for more than a few weeks
- A mass that is growing in size, changing in color, or becoming painful
- Severe localized fingertip pain with cold sensitivity (suspect glomus tumor)
- A firm palmar or finger lump that limits motion or grip
- An old ganglion cyst that has recurred after aspiration
- A mass associated with numbness, tingling, or weakness in the fingers
- Concern for cancer because of personal history or any of the red flag features listed above
Call promptly or seek emergency care for:
- A mass with overlying ulceration, drainage, or rapidly expanding redness
- A mass that becomes acutely painful with skin color change
- A pulsatile mass (may suggest aneurysm)
- A mass after recent trauma with new neurological deficits
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Dupuytren's Contracture: nodules in the palm associated with palmar fascial fibromatosis. The nodules are benign but produce contracture rather than a simple mass.
- Trigger Finger: a small palpable nodule at the A1 pulley. Easily distinguished from a true mass by the catching mechanism.
- Hand and Wrist Arthritis: bony enlargements (Heberden's and Bouchard's nodes) at the finger joints can be confused with masses but are osteophytes from underlying arthritis.
- Hand and Finger Fractures: chronic post-fracture callus or malunited bone can produce a palpable mass that mimics a tumor on examination.
- Guyon's Canal Syndrome: a ganglion cyst within Guyon's canal is a recognized structural cause of ulnar nerve compression at the wrist.
From the Blog
- How to Tell a Ganglion Cyst from a Tumor: features that distinguish benign cysts from concerning masses.
- Mucous Cysts: Why They Appear: the DIP osteoarthritis connection and the nail groove sign.
Watch: Hand mass and tumor education
Short videos from Dr. Loredo's YouTube and Instagram channels.