Cold injures the hand along a spectrum — from non-freezing cold injury and cold-induced nerve damage in people who work in freezers and cold storage, all the way to true frostbite, where tissue actually freezes and the small blood vessels clot off afterward. Most of the cold injuries Dr. Loredo treats are work injuries: contact with frozen product and cold metal, hours in cold storage and meat and food processing rooms, and cryogenic exposures like liquid nitrogen. Others come from a Texas ice storm or a night outdoors. Dr. Loredo provides both acute cold-injury care and, when tissue is lost or scarred, late reconstruction. The first hours matter enormously — and so do the years afterward, because cold sensitivity and numbness can persist long after the hand looks normal.
What Cold Actually Does to the Hand
Cold injury is not one condition. It is a spectrum, and the occupational end of it is the part almost nobody writes about.
Non-freezing cold injury. Prolonged exposure to cold that is above freezing — wet, chilled, hours long — damages nerves and small vessels without ever forming ice. It is the same process historically called trench foot or immersion foot, and the hand version is real and is exactly what happens to people who spend shifts in cold, wet conditions with saturated gloves. The hand may look almost normal and still be numb, clumsy, painful, and permanently cold-sensitive.
Cold-induced neuropathy and vasospasm. Repeated cold exposure — day after day, shift after shift — produces chronic numbness, tingling, blanching, pain, and reduced dexterity. This overlaps heavily with Raynaud's phenomenon and can be triggered or unmasked by cold work.
Frostbite — true freezing. This injures in two distinct waves, and the second wave explains the whole treatment strategy.
- Wave one — the freeze. Below roughly −0.55°C, ice crystals form in the fluid outside the cells. Water is drawn out of the cells to join the growing crystals, so cells shrivel and their internal chemistry becomes toxically concentrated. With faster or deeper freezing — contact with frozen metal, frozen product, or a cryogenic liquid — ice forms inside the cells and tears them apart. Membranes rupture.
- Wave two — the thaw, and this is the one that costs fingers. On rewarming, blood returns to vessels whose linings the freeze destroyed. They leak, swell, and then thrombose. Inflammatory mediators drive further vasoconstriction and clotting. Tissue that survived the freeze then dies from progressive microvascular thrombosis over hours to days. Repeated freeze–thaw cycles multiply this damage dramatically — which is why refreezing is catastrophic.
Why the hand: enormous surface-area-to-volume ratio; in cold, the body vasoconstricts the periphery to protect the core, and the hand is deliberately sacrificed for the heart and brain; fingertips have essentially no muscle to generate heat and minimal insulating fat; the tendons, joints, and neurovascular bundles sit just under thin skin, and nerve tissue is exquisitely cold-sensitive, which is why numbness, cold intolerance, and chronic pain persist for years even in hands that survive intact. Frostbite tends to be symmetrical and multi-digit — it rarely takes just one finger. Contact injury is the exception: it takes whatever touched.
How Cold Injures the Hand at Work: The Mechanisms We See
Most of the cold injuries we treat are work injuries. These are the specific mechanisms we see most.
Direct contact with frozen or very cold objects and surfaces (contact frostbite)
This is the most under-recognized mechanism in the entire category. Cold metal and frozen product conduct heat out of the hand far faster than cold air, so freezing is local, fast, and deep — and often happens in seconds, at temperatures where the air alone would never hurt you. A bare or thinly gloved hand on a frozen rail, a cold evaporator coil, a frozen carcass, a block of frozen product, a rack, a hook, or a cold tool can freeze skin before there's time to react. The hand can stick to the surface, which both extends the exposure and tears skin on removal.
Working in cold environments — cold storage, freezer rooms, meat and food processing
This is the biggest volume. Meat and food processing work in particular combines nearly every risk factor at once: sustained hours at or below freezing; wet hands and saturated gloves (wet hands lose heat roughly 25 times faster than dry hands); constant handling of frozen and refrigerated product with thin gloves, because thick gloves cost the dexterity the job requires; repetitive, forceful gripping that already stresses the hand's nerves and vessels; and air movement in blast freezers and chill rooms adding wind chill on top. The result is a spectrum: from non-freezing cold injury and chronic cold-induced neuropathy through contact frostbite on frozen product and metal.
Handling frozen or refrigerated laboratory and shipping equipment
Racks, cryovials, cold blocks, dry-ice-packed shipments, and equipment brought in cold from storage. These are handled reflexively and often bare-handed, and their surfaces can be far colder than a home freezer.
Cryogenic exposure — liquid nitrogen, compressed and liquefied gases, and cryogenic liquids
Liquid nitrogen is roughly −196°C (−320°F). It, and other cryogenic liquids and rapidly expanding compressed gases, cause near-instantaneous, deep freezing — and they do so in ways that catch people out: a splash does not feel wet or "cold" in a normal way, and can be shrugged off in the moment; vapor and the Leidenfrost effect create the false impression that a splash "rolled off," while a glove, cuff, or sleeve that traps the liquid against skin produces a devastating injury; cold-embrittled or frost-covered metal — a dewar, a hose, a valve, a fitting — will freeze a bare hand on contact; expanding compressed gas at a leak or a fitting flashes to well below freezing; and volatile liquids at low ambient temperature — gasoline, fuel, solvents, refrigerant — behave the same way, evaporating off skin at well below freezing and not feeling cold going on.
Settings: laboratory and research, welding gas supply, HVAC and refrigeration, cryotherapy and dermatology supply, food processing (cryogenic freezing tunnels), and industrial gas handling.
And outside of work
Ice storms and hard freezes, hours outdoors, a stalled vehicle, working on pipes or a generator in a power outage, hunting and fishing, motorcycle riding, mountaineering.
North Texas is not exempt. Recent winter storms have produced cold injuries across DFW — in a region where most people don't own real cold-weather gloves, and where a multi-day power loss puts people outside working on pipes, generators, and vehicles.
Individual risk factors that shrink your margin: alcohol, smoking and nicotine, Raynaud's phenomenon, peripheral vascular disease, diabetes and peripheral neuropathy, prior cold injury, beta-blockers, constricting gloves or rings, and age extremes.
Frostbite Classification: The Four Degrees
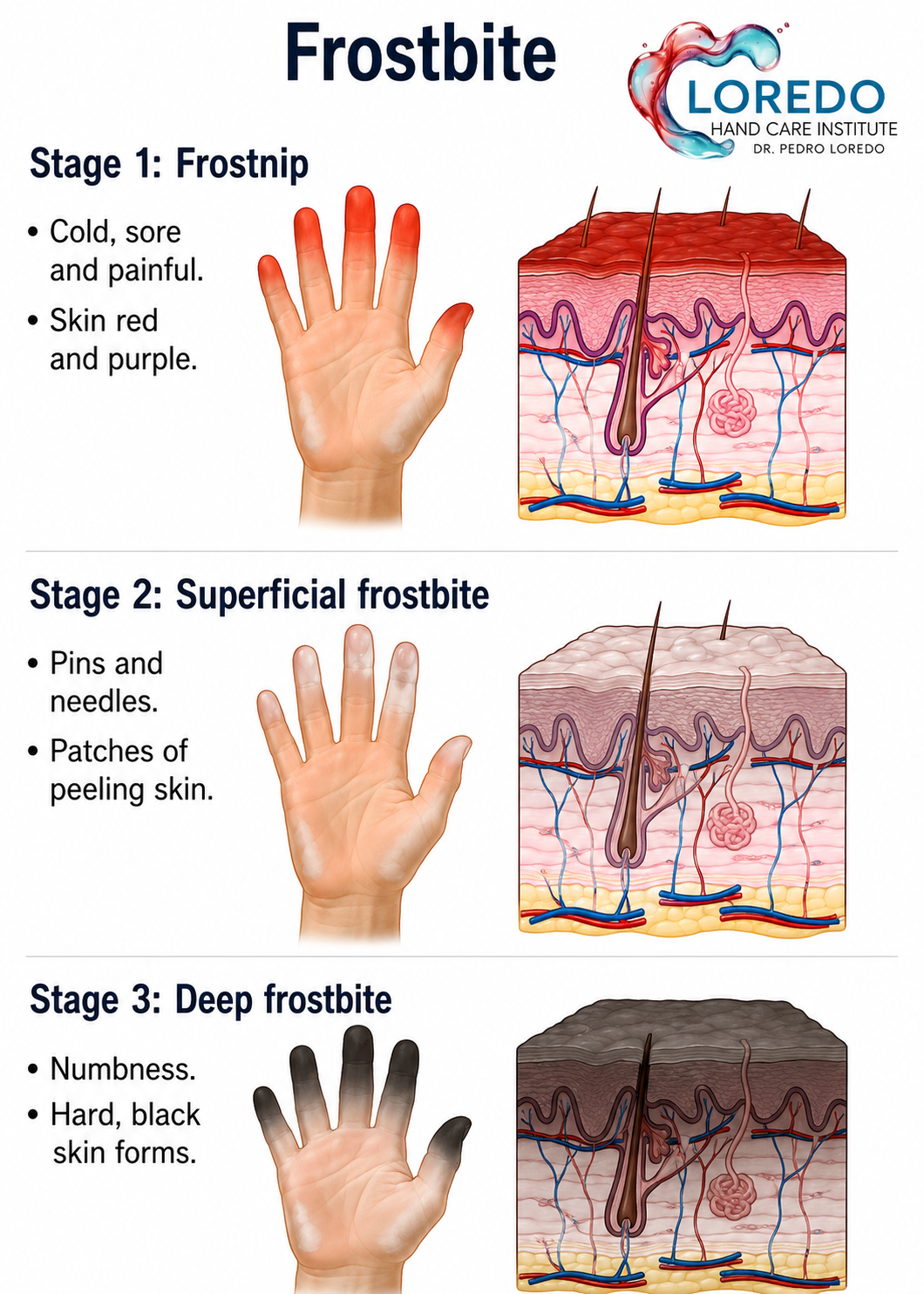
Frostbite is graded by depth, much like a burn. The initial appearance is unreliable — a frozen hand looks similar regardless of severity, and the true grade only becomes clear after rewarming, and often not fully for days to weeks.
| Degree | Depth | After rewarming | Prognosis |
|---|---|---|---|
| First degree ("frostnip") | Epidermis only | Numb central white or waxy plaque with surrounding redness and swelling; no blisters | Excellent — no tissue loss |
| Second degree | Epidermis + superficial dermis | Clear or milky blisters within 24 h, extending to the fingertips | Good — usually heals without amputation; may leave cold sensitivity |
| Third degree | Full thickness of skin + subcutaneous tissue | Hemorrhagic (dark, blood-filled) blisters, blue-grey skin | Guarded — tissue loss likely |
| Fourth degree | Through muscle, tendon, and bone | Mottled deep red-blue or purple, no blistering, hard woody tissue | Poor — mummification and amputation expected |
The single most useful clinical rule: blisters that reach all the way to the fingertips are a good sign. Blisters that stop proximally — or a hard, mottled digit that forms no blisters at all — is a bad sign; it means there wasn't enough perfusion even to raise a blister. A simpler scheme divides frostbite into superficial (1st–2nd degree, tissue loss unlikely) and deep (3rd–4th degree, tissue loss expected). Note that non-freezing cold injury sits outside this table entirely — it can produce a hand that looks nearly normal and is nonetheless numb, painful, weak, and permanently cold-intolerant.
Symptoms and Warning Signs
Early, in the cold: numbness, clumsiness, pins and needles, a hand that has stopped hurting, waxy or white skin, loss of fine dexterity.
After rewarming: intense pain, swelling, redness or mottling, blisters (clear = better; dark and blood-filled = worse), tissue that stays hard, purple, or blue-grey, or that never blisters at all.
Chronic / occupational: numbness and tingling that persists between shifts, hands that ache all winter, blanching or color change on cold exposure, hypersensitivity, altered sweating, dropped tools and lost pinch, stiffness and joint pain months to years later.
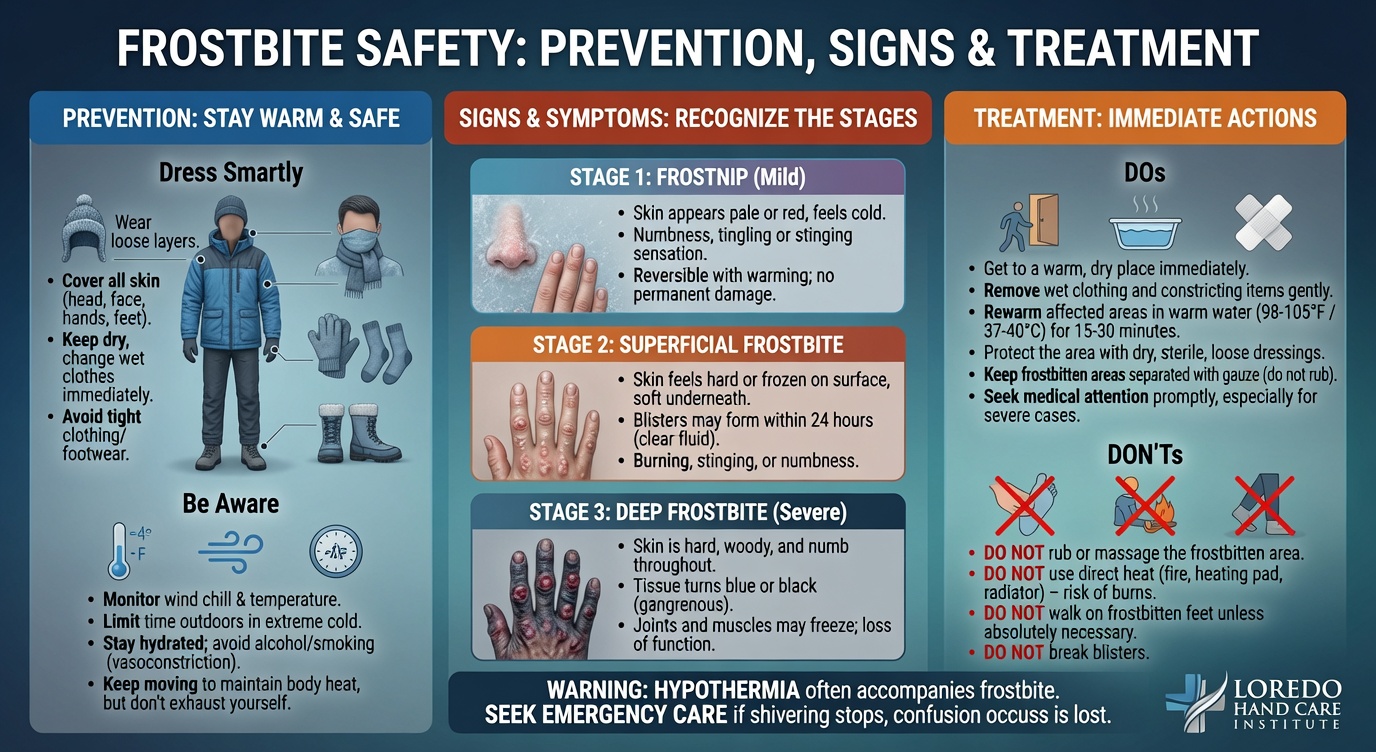
Field Treatment: Rewarming, and the Rules That Save Fingers

✅ DO — rapid rewarming. Immerse the hand in circulating water at 37–39°C (98–102°F) for 15–30 minutes, until the tissue is red-purple and pliable. Use a thermometer if at all possible; frostbitten skin is numb and cannot tell you it's being scalded. Rewarming hurts intensely — expect that meaningful pain medication will be needed.
❌ DO NOT rub, massage, or rub with snow. The tissue is full of ice crystals. Rubbing drags them through the cells like broken glass.
❌ DO NOT rewarm if there is any chance of refreezing. A frozen hand is better off staying frozen than thawing and refreezing. If you cannot guarantee the hand stays warm, keep it frozen, protect it from trauma, and get to help.
❌ DO NOT use dry heat. No campfires, heaters, stoves, hair dryers, engine blocks, or — on a job site — a heat gun or a steam line. Numb tissue cannot feel a burn.
❌ DO NOT use the hand once it's thawed. Thawed tissue is fragile.
Other measures: remove wet gloves and constricting rings immediately; ibuprofen (it blocks the thromboxane pathway driving post-thaw thrombosis); protect the hand in loose, dry, bulky padding with the fingers separated; elevate; no smoking, no alcohol; warm fluids; get to a hospital.
If a hand is stuck to a frozen surface: do not pull it free — pour warm (not hot) water over the contact point to release it.
Cryogenic splash: flood the area with large volumes of warm water immediately, and remove any clothing or glove that has trapped the liquid — trapped cryogen keeps freezing.
How the Diagnosis Is Made
Frostbite is diagnosed clinically, but the extent of injury cannot be judged by looking at the hand — that is the central problem. The old teaching was "wait for demarcation." That remains appropriate for superficial frostbite, but for deep frostbite it has been substantially replaced by early perfusion imaging.
- History: exposure temperature and duration, wind and wetness, time frozen, whether and how the hand was rewarmed and whether it refroze, alcohol and smoking, comorbidities, tetanus status, hand dominance — and the exact work exposure: the surface or substance, the temperature, the contact time, the glove worn, the shift length.
- Examination after rewarming: color, capillary refill, sensation, blister type and how far distally the blisters extend; tissue pliability; digit-by-digit assessment.
- Serial photography — essential for tracking demarcation over weeks, and essential to the record in a work claim.
- Technetium-99m (Tc-99m) triple-phase bone scan — the workhorse for assessing tissue viability in deep frostbite. Performed within the first 24–48 hours it identifies absent perfusion and can predict the eventual amputation level weeks before the hand shows you.
- Angiography (CT or catheter) — used urgently in severe frostbite to demonstrate distal arterial occlusion and establish candidacy for thrombolysis.
- MRI/MRA — can define the line between viable and nonviable tissue.
- Nerve testing — nerve conduction studies and sensory testing where non-freezing cold injury or cold-induced neuropathy is the question. Also used to separate cold injury from coexisting carpal tunnel syndrome, which cold work aggravates.
- Labs: CBC, chemistry, coagulation studies, CK, and a core temperature — hypothermia must be identified and treated first.
Treatment: Acute Care
Dr. Loredo manages cold injuries of the hand from the acute phase through full reconstruction. Deep frostbite and hypothermia are stabilized at a hospital first — see When to Call the Doctor below — and are then managed here for the hand-specific work.
- Treat hypothermia first. Always. The core comes before the hand.
- Rapid rewarming — 37–39°C circulating water for 15–30 minutes, with adequate analgesia (this frequently requires opioids).
- Ibuprofen, typically 400–600 mg every 8–12 hours, to inhibit the thromboxane-driven vasoconstriction and thrombosis of the reperfusion phase.
- Tetanus prophylaxis.
- Blister management: clear blisters are commonly aspirated or debrided; hemorrhagic blisters are generally left intact.
- Topical aloe vera under dressings in most standard protocols.
- Elevation and splinting, fingers separated and padded, no use of the part.
- Thrombolysis (tPA). In deep (3rd–4th degree) frostbite where imaging confirms distal arterial occlusion, tissue plasminogen activator can dissolve the microvascular clot and restore flow to tissue that would otherwise die. The window is generally within 24 hours of rewarming. This is why deep frostbite belongs in an emergency department today, not in an office appointment next week.
- Vasodilators and adjuncts (iloprost where available, nifedipine, pentoxifylline, sympathetic blockade) are used in some protocols.
- Escharotomy or fasciotomy. Dr. Loredo performs escharotomy and fasciotomy if a constricting eschar or compartment syndrome develops with reperfusion swelling.
Treatment: Surgery, Salvage, and Late Reconstruction
The governing principle in frostbite surgery is patience. Unlike a burn, frostbite is not an early-excision injury. "Frostbite in January, amputate in July" remains largely sound: tissue that looks black and dead is often a superficial eschar over a viable finger, and early amputation reliably takes more than it needs to.
- Watchful waiting and demarcation. Over 1–3 months, nonviable tissue mummifies and a clear line forms between living and dead tissue. Bone scan can shortcut this timeline by predicting the level far earlier.
- Early surgery only for specific indications: infection or wet gangrene, sepsis, or compartment syndrome. Infection converts patience into an emergency.
- Debridement of clearly nonviable tissue and eschar once the line is established.
- Skin grafting for granulating wounds after eschar separation.
- Flap coverage, including local, regional, and free tissue transfer using microsurgery, when tendon, joint, or bone is exposed and length is worth preserving — particularly the thumb. Dr. Loredo is fellowship-trained in hand surgery and microsurgery at the Christine M. Kleinert Institute.
- Amputation and stump revision when tissue is truly nonviable — preserving every millimeter of length that will support a healthy, sensate, durable, pain-free stump, especially for the thumb and index finger. Thumb reconstruction is considered where the thumb is lost.
- Where surgery is performed. Operative cold-injury care is carried out at Methodist Southlake Medical Center in Southlake or Crescent Medical Center Lancaster in Lancaster.
- Late reconstruction: neuroma management for painful stumps, contracture release, tenolysis, joint reconstruction, nail bed deformity.
- Long-term sequelae management: chronic cold intolerance, hypersensitivity, chronic pain and CRPS, frostbite arthritis, and — in children — growth plate injury with permanent digital shortening and angular deformity.
- For non-freezing and chronic occupational cold injury, the work is different: nerve evaluation, symptom and pain management, protection strategy, treatment of coexisting compression neuropathy, therapy for dexterity and grip, and an honest, documented assessment of what the hand can tolerate — which frequently drives the work-restriction conversation.
No outcome is guaranteed. Frostbite outcome is largely determined in the first hours — by the depth of the freeze, whether refreezing occurred, and whether the tissue was reperfused in time. Reconstruction can rebuild what survived; it cannot restore what was lost at the moment of injury.
Recovery Timeline
General expectations only; individual courses vary widely with depth.
- Hour 0–2: Out of the cold. Hypothermia assessment and treatment, rapid rewarming, analgesia, ibuprofen. Refreeze prevention.
- Hour 2–24: The decision window. Perfusion imaging or angiography in suspected deep frostbite; thrombolysis if indicated. Blisters begin to form.
- Day 1–3: Blisters mature. Swelling peaks. Splinting and elevation.
- Week 1–2: Superficial frostbite begins to heal; skin peels. Deep frostbite begins to form black eschar.
- Week 2–6: Eschar hardens and mummifies. Demarcation begins to become visible.
- Month 1–3: Demarcation completes. Definitive surgery — debridement, grafting, flap, or amputation at the preserved level — is planned here.
- Month 3–12: Wound healing, hand therapy, strengthening, stump maturation.
- Beyond 12 months: Cold intolerance, hypersensitivity, numbness, and sweating changes commonly persist for years and are frequently permanent. Prior cold injury permanently lowers your threshold for the next one — this must be addressed honestly in the return-to-work plan.
Work Injuries and Workers' Compensation
Most of the cold injuries we treat are work injuries, and cold injury claims are fought more often than almost any other mechanism — because they are poorly understood, because the hand often looks normal, and because the damage frequently accumulates over shifts instead of arriving as one dramatic event. We accept referrals from the ER, urgent care, primary care, and directly from employers and case managers.
What we do on a comp case:
- Coordinate directly with your adjuster, case manager, nurse case manager, and employer.
- Document the exposure precisely — the surface or substance and its temperature, the contact time, the shift length, the glove or PPE worn, whether the hand was wet, whether it was a single contact or a cumulative exposure. In a cold injury claim, that detail is the causation argument.
- Photograph serially from the first visit through demarcation and healing.
- Objectively test the nerve where the injury is neuropathic rather than visible.
- Issue clear, specific work status and restrictions — including, where it applies, restriction from cold exposure, which is the restriction most often omitted.
- Plan return to work realistically with the employer — grip, pinch, dexterity, tool use, glove tolerance, and cold tolerance, which may be permanently reduced.
- Handle MMI and impairment rating at maximum medical improvement.
We also participate in the VA Community Care Network (MISSION Act) for eligible Veterans, and se habla español — which matters in this category, since a large share of cold storage and food processing workers are more comfortable describing their injury in Spanish.
(See Workers' Compensation Injuries.)
Injured outside of work? You are just as welcome. Ice storm exposure, a night outdoors, a stalled car, hunting or fishing, a hand stuck to something frozen at home — same evaluation, same care. Call the office.
Frequently Asked Questions
I work in a freezer / meat plant and my hands are always numb. Is that just part of the job?
No. That's the single most important thing on this page. Hands that go numb, clumsy, or painful in the cold and don't fully recover between shifts are describing a cold injury in progress — sometimes non-freezing cold injury, sometimes cold-induced nerve damage, sometimes both, and sometimes on top of a nerve compression that the cold and the repetitive gripping have aggravated. It can happen without a single dramatic moment and without your skin ever looking abnormal, which is exactly why it gets dismissed. The damage is cumulative, and the cold sensitivity it leaves behind is frequently permanent. Get evaluated while it's still early. Bring us the specifics: the temperature, the hours, the gloves, whether your hands stay wet.
I splashed liquid nitrogen on my hand and it seemed to roll right off. Do I still need to be seen?
Yes — and please go now, not tomorrow. Liquid nitrogen is around −196°C (−320°F). A splash on exposed skin can genuinely vaporize off with minimal injury, which is the reassurance that gets people into trouble. What causes the devastating injuries is liquid that gets trapped — inside a glove, in a cuff, under a sleeve, in a shoe — because it keeps freezing against skin that cannot feel it. The same is true of touching frost-covered metal on a dewar or a line. Cryogenic injury freezes deep and instantly, and the surface can look far milder than what's underneath. Flood the area with warm water, get any trapped clothing off, and be evaluated the same day.
Should I rub my hands or put them in hot water?
No to both. Never rub frostbitten tissue — it's full of ice crystals, and rubbing drags them through the cells and shreds tissue that might have survived. Rubbing with snow is actively harmful. And not hot water: use warm water at 37–39°C (98–102°F) — body temperature, comfortable on an unaffected hand. Frostbitten skin is numb and cannot tell you it's being scalded, so people burn themselves on top of the frostbite regularly. Use a thermometer if you have one. No campfires, heaters, hair dryers — and on a job site, no heat guns and no steam lines.
My fingers turned black. Do I lose them?
Not necessarily, and this is one of the most important things to know about frostbite. Black eschar can be a superficial shell over a living finger. The traditional teaching — "frostbite in January, amputate in July" — exists precisely because surgeons who operated early kept taking more tissue than they needed to. We generally wait 1 to 3 months for a clear line to form, which preserves the maximum possible length. A Tc-99m bone scan can often predict the eventual level far earlier than the hand shows it. The one thing that forces our hand is infection — if the tissue gets infected, patience stops being an option and we operate.
My hands survived, but they're cold and painful all the time now. Is that permanent — and can I go back to my job?
Often, to some degree, yes — and I'd rather tell you honestly than have you think something has gone wrong. Cold intolerance, hypersensitivity, patchy numbness, altered sweating, and aching in cold weather are the most common long-term consequences of cold injury, and they can last years. Nerve tissue is exquisitely cold-sensitive and recovers slowly and incompletely. Some of it improves over the first year or two. What we can treat are the specific, fixable pieces — a painful neuroma, a stiff joint, a contracture, frostbite arthritis — plus a real strategy for managing the cold sensitivity. As for your job: your hands are now permanently more vulnerable, and prior cold injury lowers your threshold for the next one. If your work is cold work, that is a real conversation about restrictions, and it's one we'll document clearly for your employer and your carrier rather than leaving you to have it alone.
When to Call the Doctor
Call our office for evaluation if you have:
- Any cold injury, once you are out of the acute emergency phase
- Fingers that stay numb, discolored, or painful after cold exposure
- Numbness, tingling, clumsiness, or pain in your hands from working in cold storage, a freezer, or a processing plant — even if the skin looks completely normal
- Blisters, eschar, or a wound that isn't healing
- A frostbite injury that has demarcated and needs a plan
- Cold intolerance, hypersensitivity, or chronic pain in a previously injured hand
- A painful spot or nodule in a stump (possible neuroma)
- Stiffness, contracture, or joint pain months to years after cold injury (possible frostbite arthritis)
- Repeated cold-triggered white-and-numb fingers — this may be Raynaud's and should be evaluated
- A prior cold injury limiting your work or daily life — even years later
- A child with a prior frostbite injury whose finger appears to be growing abnormally
🚨 Go to the emergency department immediately — call 911 if the person is confused, drowsy, or has stopped shivering — for:
- Suspected hypothermia — confusion, slurred speech, clumsiness, drowsiness, or shivering that has stopped. This outranks the hand every time.
- Skin that is white, waxy, hard, and completely numb
- Tissue that is hard and woody and does not indent
- Any hemorrhagic (dark, blood-filled) blister
- Fingers that remain mottled, purple, or blue-grey after rewarming, or that form no blisters at all
- Any suspected deep frostbite — same day. The thrombolysis window is generally within 24 hours of rewarming
- Cryogenic exposure — liquid nitrogen, compressed or liquefied gas, refrigerant — or fuel or solvent splash. These freeze deeply and instantly, and the skin can look deceptively mild
- Fever, spreading redness, foul drainage, or worsening pain — possible infection
- Frostbite in a child, or in anyone with diabetes, peripheral vascular disease, or Raynaud's
Deep frostbite is time-critical. The treatment that can save fingers has a window measured in hours from rewarming. Do not wait for an office appointment to find out how bad it is. For any medical emergency, call 911 or go to the nearest emergency department.
Prevention
Cold work — freezer, cold storage, meat and food processing:
- Dry hands are everything. Wet hands lose heat about 25 times faster. Carry spare gloves and change them the moment they're wet.
- Never handle frozen product or cold metal bare-handed, even for "just a second." Contact freezing is fast, local, and deep.
- Do not trade all your insulation for dexterity. If the job needs thin gloves, it needs scheduled warm-up breaks.
- Rotate out of the cold room. Cumulative exposure is what produces the numb, clumsy, permanently cold-sensitive hand.
- Take numbness seriously the first time. A hand that goes numb every shift and doesn't fully recover between shifts is an injury in progress. Report it.
Cryogens and compressed gas:
- Use cryogenic-rated gloves — loose, so they can be thrown off instantly — plus a face shield and sleeves.
- Never tuck sleeves into gloves or wear a cuff that can trap liquid against skin. Trapped cryogen is what turns a splash into an amputation.
- Never touch frost-covered or cold-embrittled metal — a dewar, hose, valve, or fitting — with a bare hand.
- Treat liquid nitrogen at roughly −196°C (−320°F) as what it is. It does not feel like it's hurting you until it already has.
- Handle fuel, solvents, and refrigerant in cold weather with the right gloves.
Outdoors and at home:
- Mittens beat gloves — fingers keep each other warm. Layer, cover every square inch, and respect wind chill.
- No alcohol in the cold. Don't smoke — nicotine constricts exactly the vessels you need.
- Remove rings and anything constricting before cold work.
- Never touch bare metal in a hard freeze.
- Know the early warning: numbness, clumsiness, waxy white skin, or a hand that has stopped hurting. Get warm then, not later.
- If you have Raynaud's, diabetes, neuropathy, or prior cold injury, your margin is much smaller than everyone else's.
- In a Texas ice storm: don't work on pipes, generators, or a stalled car in light gloves with no plan.
Related Conditions
- Hand and Upper Extremity Burns: the opposite end of the thermal injury spectrum — Dr. Loredo treats both acute and late reconstruction for both cold injury and burns, and both categories are heavily occupational.
- Raynaud's Disease: the most important companion page. Cold-triggered vasospasm is frequently confused with frostbite, sharply lowers cold tolerance, is unmasked by cold work, and is a genuine risk factor for true freezing injury.
- Workers' Compensation Injuries: most of the cold injuries we treat are work-related — cold storage, meat and food processing, cryogenic handling, refrigeration, and outdoor cold exposure.
- Carpal Tunnel Syndrome: cold, wet, repetitive-gripping work aggravates nerve compression, and the two frequently coexist.
- Hand and Finger Fractures: cold exposure often accompanies trauma, and cold injury can complicate an injured hand.
- Dupuytren's Contracture: a separate disease, but the same late problem of fingers held in fixed flexion and the same reliance on release and hand therapy.