Burns of the hand are among the most function-threatening injuries in the body — the skin on the back of the hand is barely a millimeter thick, and the extensor tendons and joints lie directly beneath it. Most of the hand burns Dr. Loredo treats are work injuries: hot liquids and oil, steam and vapor, and hot surfaces and flame. Many others happen at home, in the kitchen and the garage. Dr. Loredo provides both acute burn care and, when scarring or contracture develops, late reconstruction. Whether your burn is a workers' compensation claim or a Saturday-afternoon accident, the goals are the same — protect depth, prevent contracture, and get the hand moving.
Why a Burn of the Hand Is Different
The hand is only about 3% of your body surface area, but virtually any meaningful burn of the hand is considered a burn that needs specialized care — no matter how small it looks. That is entirely about anatomy.
- The dorsal (back-of-hand) skin is roughly a millimeter thick, with almost no fat beneath it to insulate what lies under.
- The extensor tendons run directly under that skin. Over the PIP joint the extensor mechanism thins into the central slip and lateral bands — structures with a fragile blood supply. A deep dorsal burn can expose or destroy them and produce a boutonnière deformity.
- The joints are superficial. Full-thickness dorsal burns can expose the MCP and PIP joint capsules directly.
- The palm is a different tissue entirely — thick glabrous skin built for grip and sensation, and not replaceable by ordinary graft without losing durability and feel.
- Scar contracts across every crease it crosses. A burn crossing the wrist, the web spaces, or the volar fingers will pull the hand into a fixed posture unless it is splinted and, when necessary, released.
- Swelling and stillness are their own injury. A swollen hand held still for two weeks becomes a stiff hand whether or not the burn was deep.
The classic bad outcome is the burn claw hand: MCP joints hyperextended, PIP joints flexed, thumb pulled into the palm, web spaces obliterated. Preventing that posture is the single organizing goal of early hand burn care.
How Hand Burns Happen: Mechanisms We Actually See
Most of the hand burns we treat are work injuries. The mechanisms below are the ones that walk through our door — described the way they actually happen on a job site, in a plant, or in a kitchen.
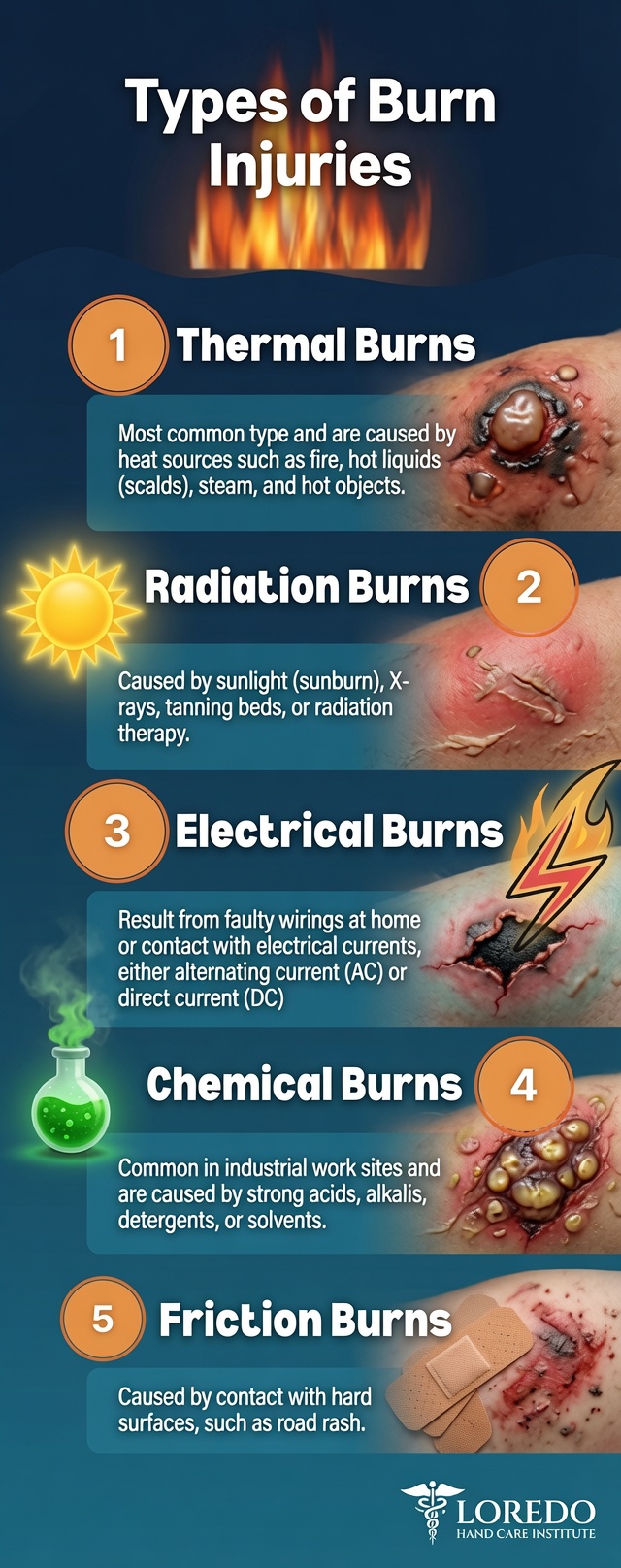
Liquid burns (scald)
- Hot water and steam-line condensate — commercial kitchens, dish pits, boiler and steam-line work, food plants.
- Hot oil and grease — fryers, griddles, oil changes, hot machine lubricant and hydraulic fluid. Oil holds heat far longer than water and burns deeper for the same splash.
- Hot chemical solution — process tanks, cleaning solutions, plating baths. A chemical and thermal injury at once.
- At home: kettles, pots, deep fryers, coffee, bathwater, a pot handle turned outward.
Vapor and steam burns
Steam carries an enormous amount of heat and condenses on the skin, dumping all of it at once. A steam burn is routinely deeper than the same temperature of dry air. Steam lines, autoclaves, pressure cookers, radiators, sterilizers, and vapor releases from valves and fittings all produce this. A steam jet under pressure can also drive vapor through a glove.
Heat, contact, and flame burns
- Contact with hot surfaces — ovens, griddles, presses, dies, molds, manifolds, weld metal, pipes, irons. Contact burns are usually deep, because the hand stays on the surface — sometimes because it's stuck, sometimes because the burn was fast enough to be painless.
- Flame and flash — torch work, grinding sparks near fuel, grill and gasoline flash, brush fires, garage fires.
- Friction burns — machinery, belts, ropes, road rash. A combined burn and abrasion.
Chemical burns
- Acids (hydrochloric, sulfuric) cause coagulative necrosis and tend to be self-limiting at the surface.
- Alkalis (lye, drain cleaner, wet cement, oven cleaner) cause liquefactive necrosis and burrow deeper over time — they are frequently far worse than they look on arrival.
- Hydrofluoric acid is its own emergency: severe pain with almost no visible skin change, while fluoride ion binds calcium and destroys tissue — and can cause fatal systemic hypocalcemia. An HF exposure is an emergency even when the skin looks nearly normal.
Electrical injury
The entry and exit wounds massively understate the damage. Current follows nerve, vessel, and muscle and cooks tissue from the inside; the hand is very often the entry point. High-voltage injury carries real risk of deep muscle necrosis, compartment syndrome, rhabdomyolysis with kidney injury, and cardiac arrhythmia. Any electrical burn is an emergency — including one that looks small.
Where these happen: commercial kitchens and food service, food and meat processing, manufacturing and fabrication, welding, plating and chemical handling, oil and gas, HVAC and boiler work, electrical trades, construction, and auto repair — plus the kitchen and the garage at home.
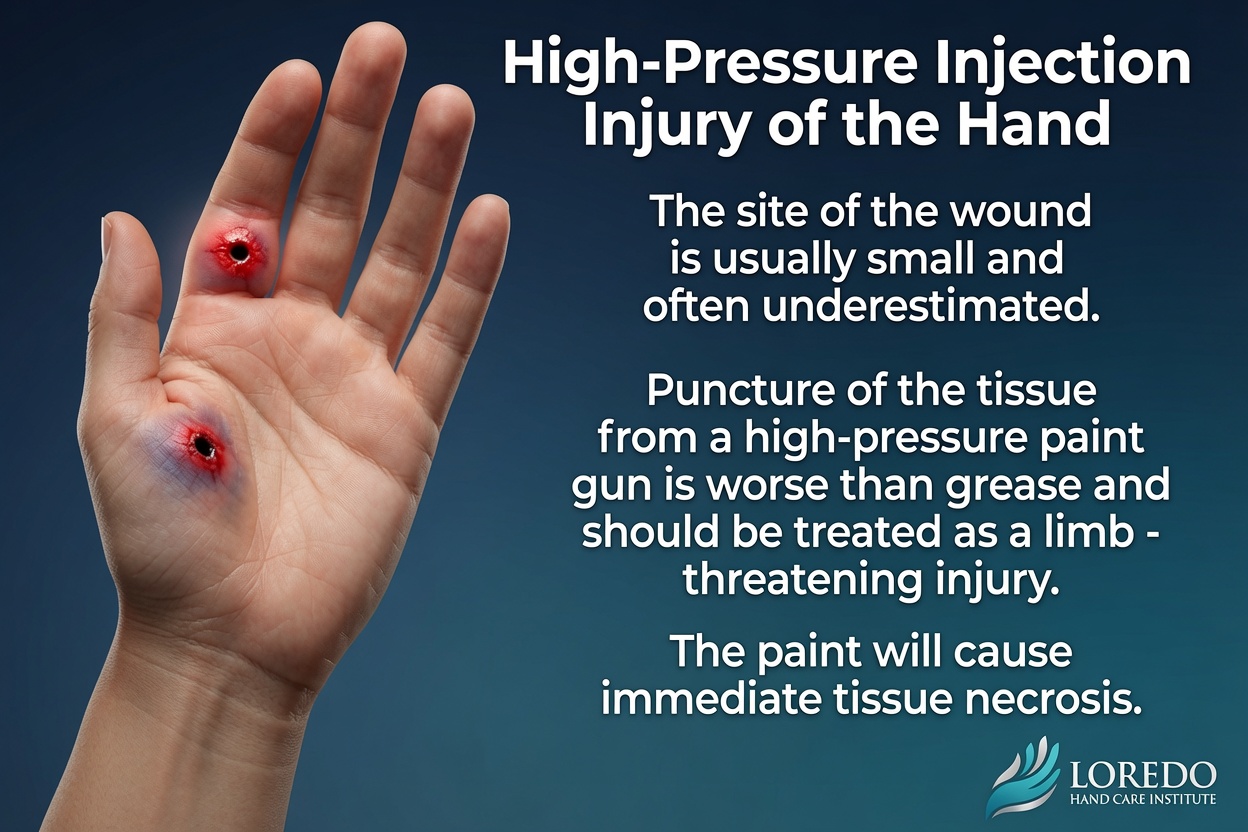
High-Pressure Injection Injury — A Surgical Emergency Easily Missed
Paint, grease, hydraulic fluid, or diesel driven through the skin by an industrial spray gun. This is not a burn, but it belongs on this page because it is frequently overlooked in the emergency department — the entry wound is a tiny, innocuous-looking pinhole, and the finger can look almost normal for the first hour. It isn't. The injected material tracks along the tendon sheaths and fascial planes, causing severe deep tissue damage far beyond what the entry point suggests.
The majority of these injuries require immediate surgical decompression and debridement. Delay dramatically raises the risk of amputation — this is one of the most time-critical injuries in hand surgery, even though it rarely looks like one at first glance.
If a spray gun has ever touched your hand, even for a second, and even if it "just felt like a bump": go to the emergency department now, or call our office immediately. Do not wait to see if it starts hurting.

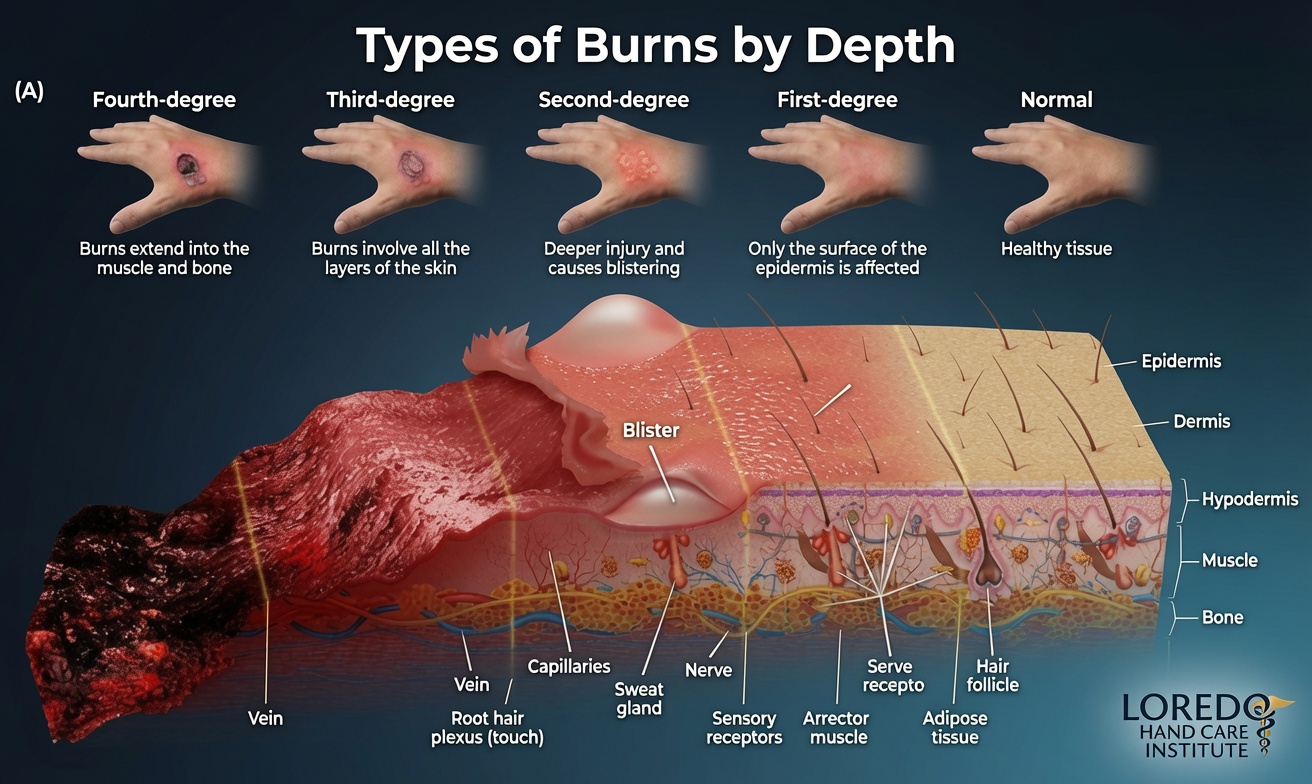
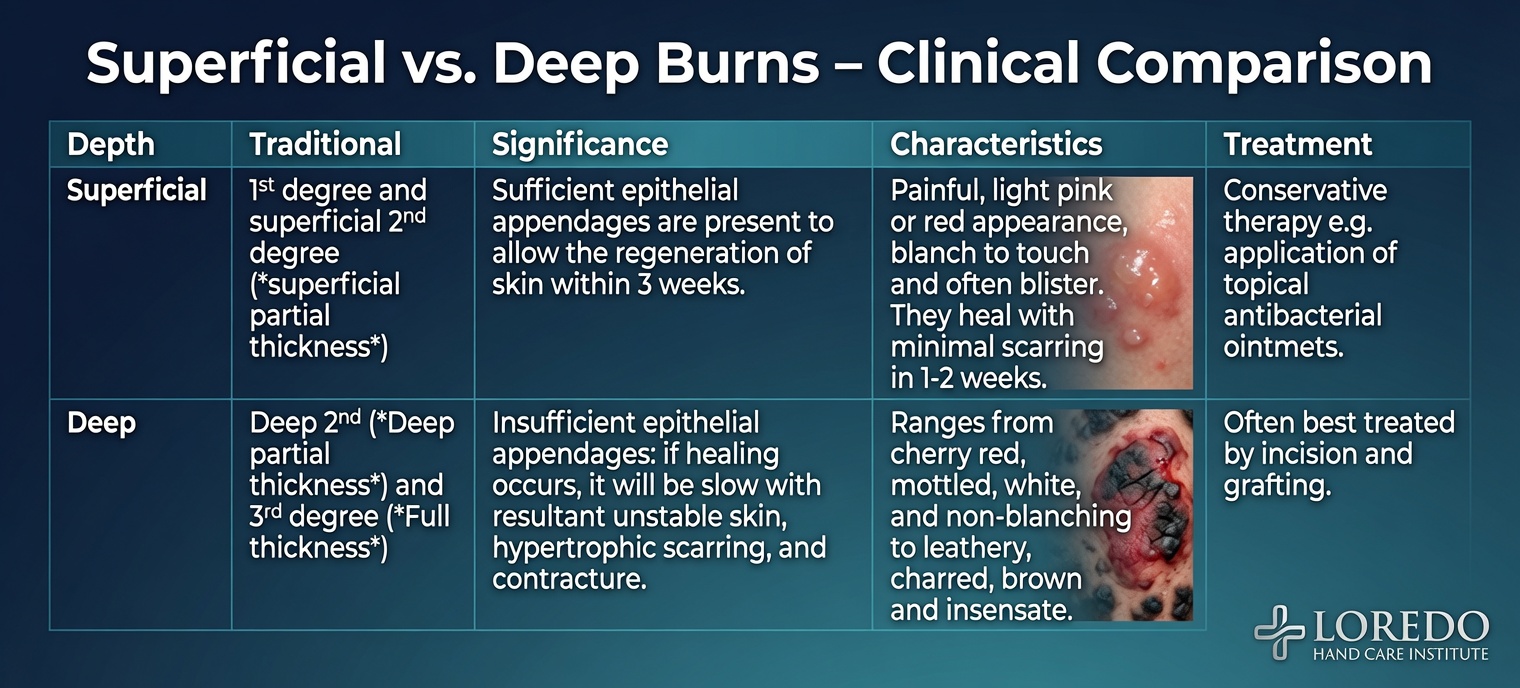
Burn Depth: How Burns Are Classified
Depth — not size — decides whether a hand burn heals or scars. Depth is also not reliable on day one. Burns "declare" themselves over 48 to 72 hours and can convert to a deeper injury.
| Depth | Older term | Appearance | Sensation | Healing |
|---|---|---|---|---|
| Superficial | First degree | Red, dry, no blisters | Painful | 3–7 days, no scar |
| Superficial partial thickness | Superficial second degree | Moist, pink, blisters, blanches briskly | Very painful | ~2–3 weeks, minimal scar |
| Deep partial thickness | Deep second degree | Mottled red/white, drier, sluggish or absent blanching | Reduced pinprick | >3 weeks; scars and contracts — often grafted |
| Full thickness | Third degree | White, waxy, leathery, or charred; dry, no blanch | Insensate | Will not heal from the edges; requires excision and grafting |
| Fourth degree | — | Into tendon, muscle, joint, or bone | Insensate | Requires flap coverage; amputation may be unavoidable |
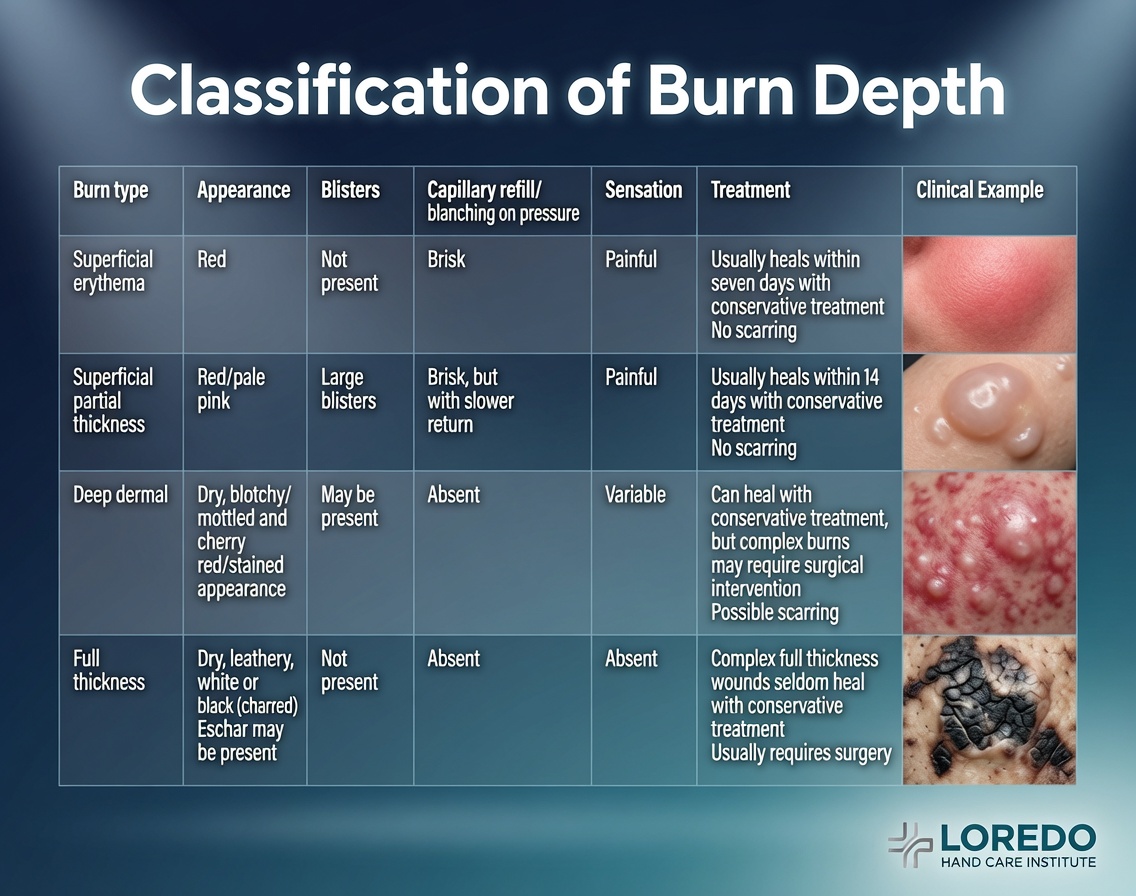
Two points that matter for the hand: Deep partial thickness is the decision point — left alone, a deep partial burn on the back of the hand will usually close, with a thick, contracting scar and a stiff hand; early excision and grafting frequently produces a better hand. And a painless burn is a worse burn — a white, leathery patch that doesn't hurt is nerve destruction, not good news.
Symptoms and Warning Signs
- Redness, blistering, weeping, or a white/waxy/leathery patch
- Numbness in the burned skin — a warning sign, not a relief
- Rapid swelling; a ring that is getting tight
- Pain that keeps increasing after the first day
- A burn that is still open or weeping after 2 weeks
- Fingers beginning to curl, stiffen, or lose motion
- A scar that is thickening, raising, reddening, itching, or tightening
- A web space closing down, or a thumb that will not come out of the palm
- Persistent cold intolerance, tingling, or a painful spot in a burn scar
- Spreading redness, fever, or foul drainage — infection
First Aid: The First Ten Minutes
- Stop the burning. Remove the source. Remove rings and watches immediately — before swelling makes it impossible. A ring on a swelling burned finger is a tourniquet.
- Cool running water for 20 minutes. Cool, not cold. Worth doing even up to three hours after the injury.
- Do not use ice. It deepens the burn.
- Do not apply butter, oil, toothpaste, or home remedies. Do not break blisters.
- Chemical burns: irrigate far longer — 30 minutes or more, much longer for alkali. Brush dry powdered chemicals off before wetting (cement, lime). Do not try to neutralize a chemical.
- Cover loosely with a clean, dry, non-adherent dressing. Elevate above heart level.
- Electrical: make sure the source is off before touching the person.
- Work injury: report it to your supervisor the same day and bring the SDS sheet or the product container.
How the Diagnosis Is Made
Hand burn assessment is clinical and serial — the burn is re-examined over days because depth evolves.
- History: agent, temperature, duration of contact, voltage and pathway for electrical, product identity and pH for chemical, time since injury, first aid given, tetanus status, hand dominance, and occupation and exact job task.
- Examination: depth by appearance, blanching, and sensation to pinprick; extent using the palm as roughly 1% TBSA; capillary refill; tendon function finger by finger; specific assessment of the web spaces and the thumb.
- Vascular and compartment assessment: pulses, Doppler, digital pulse oximetry, compartment pressures where indicated. A Doppler pulse can persist while a compartment is dying — compartment syndrome is a clinical diagnosis.
- Serial re-examination at 48–72 hours to catch burn conversion and make the graft decision.
- X-ray for suspected fracture, foreign body, or injected material.
- Labs for electrical injury: CK, myoglobin, renal function, EKG.
- Photographic documentation — for tracking healing and, in work injuries, for the record.
Treatment: Acute Care
Dr. Loredo manages hand burns from the acute phase through full reconstruction. Super-acute and major burns are stabilized at a burn center first — see When to Call the Doctor below — and are then managed here for the hand-specific work.
- Wound care: cleansing, careful debridement of loose devitalized skin, topical antimicrobial or a modern silicone/foam dressing, tetanus prophylaxis as indicated. Blister management is individualized.
- Escharotomy. Dr. Loredo performs escharotomy for circumferential full-thickness burns. A rigid, non-elastic eschar acts like a tourniquet as the limb swells beneath it, producing compartment syndrome; longitudinal releasing incisions along the mid-lateral lines relieve it. This is time-critical — measured in hours, not days.
- Fasciotomy for true compartment syndrome — common in electrical and crush-associated burns, and a distinct problem from eschar constriction. Dr. Loredo performs fasciotomy for burn-related compartment syndrome. Escharotomy and fasciotomy are performed at Methodist Southlake Medical Center in Southlake or Crescent Medical Center Lancaster in Lancaster.
- Chemical burns: irrigation is the treatment, continued far beyond what feels sufficient; hydrofluoric acid additionally requires calcium therapy and monitoring for systemic hypocalcemia.
- Elevation and edema control from hour one. Swelling is the enemy of the hand.
- The antideformity (safe / intrinsic-plus) splint — the most important non-operative maneuver in hand burn care: wrist extended ~20–30°, MCP joints flexed 70–90°, IP joints fully straight, thumb abducted out of the palm, web spaces held open. The natural resting posture of a swollen hand is the exact opposite — and that posture is the claw deformity.
- Early motion, as soon as the wound permits, splinted between sessions.
- Pain control sufficient to permit therapy — an under-medicated hand doesn't move.
Treatment: Surgery and Late Reconstruction
- Tangential excision and skin grafting. Deep partial and full-thickness burns are excised in layers to viable, bleeding tissue, then resurfaced. Sheet grafts (not meshed) are strongly preferred on the hand. The dorsum typically takes a split-thickness graft; the palm and volar fingers do better with full-thickness graft.
- Dermal substitutes where the bed is poor or a thicker, more pliable result is needed over tendon and joint.
- Flap coverage when tendon, joint capsule, or bone is exposed — local and regional flaps, pedicled flaps, and free tissue transfer using microsurgery. Dr. Loredo is fellowship-trained in hand surgery and microsurgery at the Christine M. Kleinert Institute.
- Contracture release — often the operation that gives a patient their hand back. Z-plasty and local flap rearrangement for linear bands; full-thickness grafting for broad contractures; web space release, particularly the first web space, to restore thumb abduction and grip; capsular release for joints that have stiffened. Release is normally timed once the scar is mature — commonly 6–12 months — unless a rapidly progressing contracture is destroying function, or a growing child requires earlier action.
- Tendon reconstruction, tenolysis, and joint reconstruction for late boutonnière deformity, extensor loss, and fixed joints.
- Amputation revision when a digit is truly nonviable, or when a stiff, insensate, painful digit is actively obstructing an otherwise good hand. That is a hard conversation and it is had honestly. A well-performed amputation with a healthy, sensate stump sometimes gives a better working hand than a preserved digit that hurts and won't move.
- Scar management — silicone sheeting, compression gloves, massage, and steroid injection for hypertrophic scar.
- Hand therapy. Dr. Loredo does not have in-house therapy and refers to dedicated certified hand therapists in the DFW area for antideformity splinting, serial splinting to stretch developing contractures, range of motion and tendon gliding, web space spacers, compression garments (frequently 12–23 hours a day for 6–12 months), scar massage and desensitization, and strengthening with a work-specific return plan. Surgery buys the opportunity; therapy determines the result.
No outcome is guaranteed. Burn reconstruction is staged. Results depend on the depth of the original injury, what structures were lost, your healing biology, and — heavily — on participation in therapy.
Recovery Timeline
General expectations only; individual courses vary widely with depth and mechanism.
- Day 0–3: Emergency care, cooling, depth assessment, release of a constricting eschar if needed. Splint applied.
- Day 3–7: Serial reassessment. The decision is made: heal on its own, or excise and graft.
- Week 1–3: Superficial partial burns close. Grafts assessed for take around days 5–7; donor site heals in roughly 10–14 days. Protected motion begins.
- Week 3–6: Wounds largely closed. Therapy intensifies. Compression garments fitted.
- Month 2–6: The scar maturation window — and the highest-risk period for contracture. Splinting and garment compliance decide the outcome here.
- Month 6–18: Scar softens and fades. Reconstruction — contracture release, web space release, tendon work — is typically planned in this window.
- Beyond 18 months: Scar generally mature. Sensation may keep recovering slowly. Staged reconstruction may continue for years in children.
Return to activity (general ranges): small superficial partial burn, days to ~2 weeks · grafted dorsal hand burn with office work, ~3–6 weeks · grafted hand burn with manual labor, ~2–4 months · flap reconstruction or electrical injury, highly variable and often several months.
Work Injuries and Workers' Compensation
Most of the hand burns we treat are work injuries, and we are set up for them. Burns are one of the most common serious occupational hand injuries in North Texas — kitchens, food and meat plants, manufacturing, welding and fabrication, chemical handling, HVAC and boiler work, oil and gas, electrical trades, and construction. We accept referrals from the ER, urgent care, primary care, and directly from employers and case managers.
What we do on a comp case:
- Coordinate directly with your adjuster, case manager, nurse case manager, and employer — including accommodating case-manager involvement in visits where appropriate.
- Document the mechanism precisely — the agent, the temperature, the exposure time, the job task, the PPE in use. In a burn claim, mechanism is causation.
- Photograph the injury serially from the first visit through healing.
- Issue clear, specific work status and restrictions — not "no use of hand," but what the hand can and cannot do, so light duty is actually usable.
- Communicate return-to-work planning with the employer, including realistic timelines for grip, pinch, tool use, heat exposure, and glove tolerance.
- Handle MMI and impairment rating when the case reaches maximum medical improvement.
- Provide the treating-surgeon record the carrier needs — depth, treatment, surgical findings, therapy course, and outcome.
We also participate in the VA Community Care Network (MISSION Act) for eligible Veterans, and se habla español — including for injured workers whose comfort language is Spanish.
(See Workers' Compensation Injuries.)
Burned at home instead? You are just as welcome, and nothing about the care changes. Kitchen scalds, grease burns, garage and grill flash burns, and oven contact burns are treated exactly the same way. Call the office.
Frequently Asked Questions
My burn doesn't hurt. Is that good?
No — it's usually the opposite. Pain means the nerve endings in the skin are still alive, which is what you want. A burn that's white, leathery, waxy, or charred and numb has typically destroyed those nerve endings, which means full-thickness injury. Painless burns need to be looked at, not shrugged off.
It happened at work. Do I have to use the doctor they send me to?
Bring the question to us and we'll walk you through it. What we can tell you plainly is that we treat workers' compensation hand injuries routinely, we accept referrals from the ER, urgent care, primary care, and employers or case managers, and we work directly with adjusters and nurse case managers. We document the mechanism and your work status the way a comp claim requires — the agent, the temperature, the exposure time, and the job task are what establish causation. Call the office at (972) 939-4974 and we'll tell you exactly what's needed. Se habla español.
My hand burn seems small — do I really need a hand surgeon?
Very likely, yes. Essentially any meaningful burn of the hand is considered a burn requiring specialized care, no matter how small the area, because the tendons and joints sit directly under paper-thin skin. A burn that would be trivial on your thigh can permanently cost you grip, pinch, or the use of a finger. The area of a hand burn tells you almost nothing. The depth and the location tell you everything.
Will I need a skin graft, and will it look normal?
It depends entirely on depth. Superficial and superficial partial-thickness burns heal on their own. Deep partial and full-thickness burns generally need excision and grafting, because leaving them to heal produces a thick, contracting scar and a stiff hand. On the hand we use sheet grafts rather than meshed grafts specifically to avoid the permanent diamond pattern and reduce contracture. Honestly: grafted skin will not look identical to your original skin — it will differ in color and texture and will always be more sun-sensitive. What we prioritize is a hand that moves, grips, and feels. Appearance is optimized, not guaranteed.
My fingers are curling in and won't straighten. Can that be fixed?
Often, yes — this is scar contracture, and it's one of the more rewarding problems in hand surgery. Burn scar shortens as it matures and pulls fingers into a fixed bend, closes down the web spaces, or traps the thumb in the palm. Dr. Loredo performs release surgery — Z-plasty, local flaps, full-thickness grafting, web space release, and sometimes joint capsule release — to restore substantial motion. Timing matters: we usually wait for the scar to mature, commonly 6 to 12 months, unless it's progressing fast or a child's growth demands earlier release. Recurrence is possible, and the splinting and therapy afterward aren't optional — they're how the result is held.
When to Call the Doctor
Call our office for evaluation if you have:
- Any burn on the hand, wrist, or fingers — even a small one
- A burn still open, weeping, or unhealed after 2 weeks
- Fingers starting to curl, stiffen, or lose motion after a burn
- A thickening, raised, red, itchy, or tightening scar
- A web space closing down, or a thumb that will not come out of the palm
- Numbness, tingling, or persistent cold intolerance in a previously burned hand
- A painful spot in a burn scar (this can be a neuroma)
- A healed burn limiting your work, grip, or daily life — even if it happened years ago
- A new sore, ulcer, or growth in an old burn scar
🚨 Go to the emergency department or call 911 immediately for:
- A circumferential burn of any finger, hand, wrist, forearm, or arm
- Increasing deep pain, severe pain on straightening the fingers, a tight, tense, numb, cold, or dusky hand — possible compartment syndrome
- Any electrical burn, including one that looks small
- Any chemical burn — irrigate with water on the way, and bring the container or SDS sheet
- Hydrofluoric acid exposure — even with minimal visible skin injury
- High-pressure injection injury (paint, grease, hydraulic fluid, diesel) — even a pinhole. This is a surgical emergency; do not wait.
- Burn with exposed tendon, joint, or bone, or charring
- Burns to the face or airway, hoarseness, soot in the nose or mouth, or trouble breathing
- Large burns, burns in a child, or burns with any other significant injury — these need a burn center
- Fever, chills, spreading redness, or foul-smelling drainage
Severe burns are time-critical. Releasing a constricting circumferential burn is measured in hours, not days. Major and super-acute burns and deep injuries belong at a burn center first — go to the emergency department or call 911, do not wait for an office appointment. For any medical emergency, call 911 or go to the nearest emergency department.
Prevention
At work:
- Wear gloves rated for the actual hazard — heat, steam, chemical, or arc-flash — not whatever gloves were in the truck. A wet or saturated glove conducts heat; it doesn't stop it.
- Treat steam and vapor as hotter than the gauge suggests. Never break a line or a fitting without confirming it's isolated and depressurized.
- Know the SDS for every chemical you touch, know where the eyewash and safety shower are, and keep calcium gluconate gel available anywhere hydrofluoric acid is used.
- Lock out, tag out. Assume every conductor is live.
- Never clean or test a high-pressure spray gun against your hand. Not once.
- Remove rings before working with machinery, heat, or electricity.
- Report a burn the same day it happens, even a small one.
At home:
- Set the water heater at or below 120°F.
- Turn pot handles inward; keep children out of the cooking zone; never carry a child and a hot liquid together.
- Dry food before it goes into hot oil, and never move a burning pan.
- Never use gasoline to start or accelerate a fire; keep the grill lid clear when igniting.
Related Conditions
- Frostbite and Cold Injury of the Hand: the opposite end of the thermal injury spectrum — Dr. Loredo treats both acute and late reconstruction for both burns and cold injury, and both categories are heavily occupational.
- Workers' Compensation Injuries: most of the hand burns we treat are work injuries; scald, steam, chemical, contact, and electrical burns are frequently compensable.
- Extensor Tendon Injury: the extensor tendons lie directly beneath the thin dorsal skin and are commonly damaged or exposed in deep dorsal burns.
- Flexor Tendon Injury: palmar burns and contractures can involve or tether the flexor system.
- Dupuytren's Contracture: a different disease, the same functional problem — fingers pulled into a fixed bend by contracting tissue, and the same reliance on release and therapy.
- Hand and Finger Fractures: machinery, electrical, and crush injuries frequently combine burns with fractures.