Hand and elbow pain can come from a nerve, a tendon, a joint, a bone, a vessel, or a soft-tissue problem. The location of the pain, what it feels like, and what makes it worse together usually identify the underlying diagnosis. This page is a triage guide. It helps you decide whether your symptoms warrant a hand surgeon evaluation, a primary care visit, or emergency care, and what you can do at home in the meantime. For specific diagnoses, follow the internal links to the dedicated condition pages.
When to See a Hand Surgeon
Direct evaluation by a hand surgeon is the right first step when your symptoms suggest a specific structural problem in the hand, wrist, or elbow.
- Numbness or tingling in specific fingers, particularly when it wakes you at night or worsens with specific positions
- A finger that catches, clicks, or locks with bending and straightening
- Persistent pain at a specific tendon or joint that has not improved over 4 to 6 weeks
- A visible mass or lump on the hand, wrist, or fingers
- A finger or wrist deformity, including a depressed knuckle, drooping fingertip, or contracted finger
- Pain after a fall or injury that has not improved over 48 to 72 hours
- Loss of grip strength or difficulty with fine motor tasks
- Joint swelling, redness, or visible joint changes
- Failed conservative care from primary care for a suspected hand or wrist condition
You do not need a referral from primary care for most insurance plans. Direct hand surgeon evaluation often shortens the path to treatment, particularly when the diagnosis is clear (carpal tunnel, trigger finger, De Quervain's, fractures).
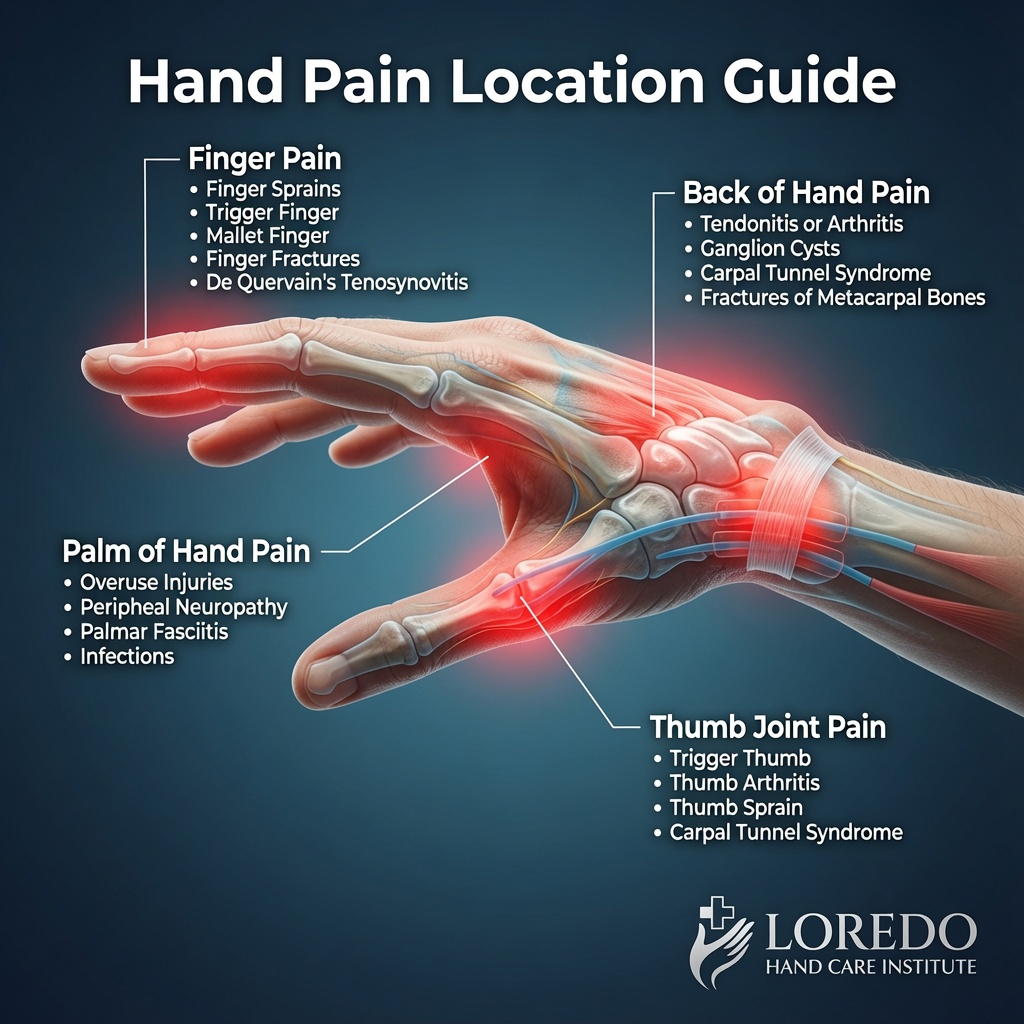
Pain by Location
Where the pain is is the strongest single hint about what is causing it.
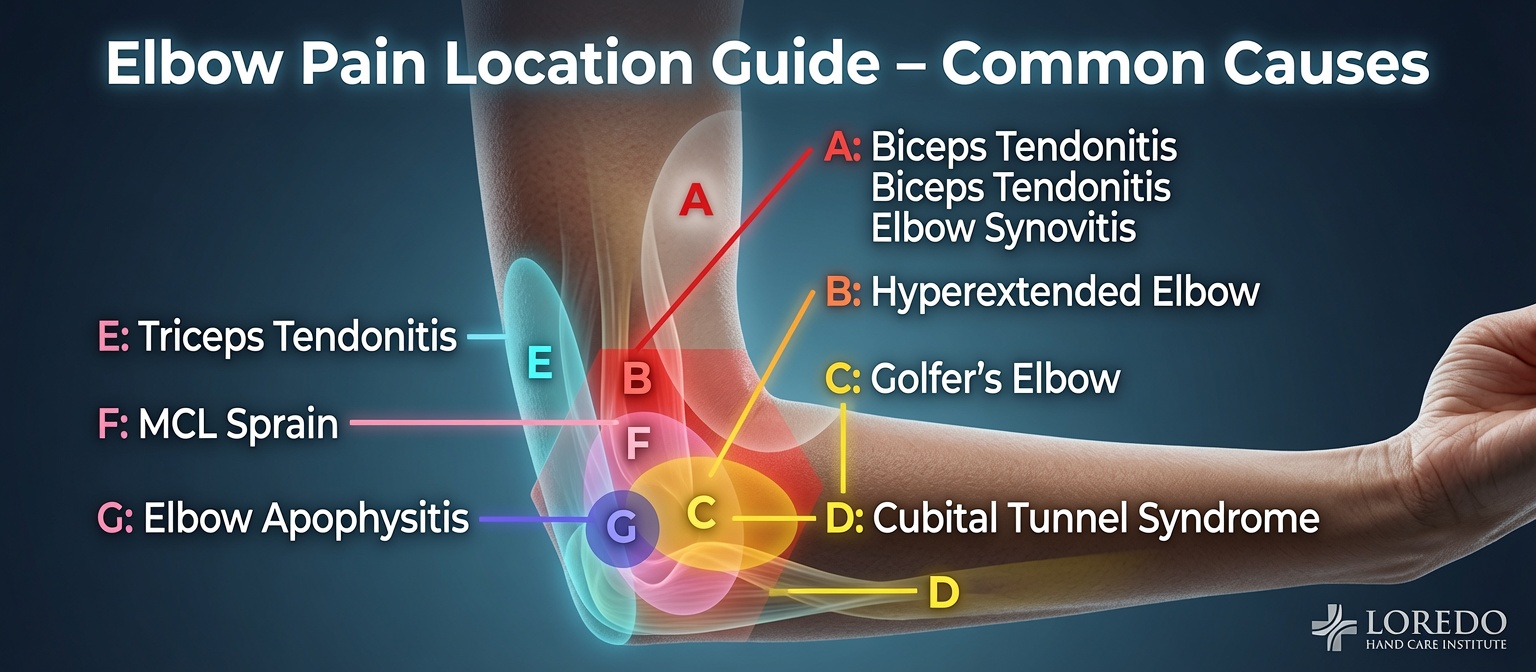
Outer (Lateral) Elbow Pain
The most common cause is tennis elbow (lateral epicondylitis), a degenerative tendinopathy at the bony bump on the outside of the elbow. Pain worsens with gripping, lifting with the palm down, and shaking hands. The closely related radial tunnel syndrome can mimic tennis elbow but localizes 4 to 5 finger-breadths distal to the bone bump.
Inner (Medial) Elbow Pain
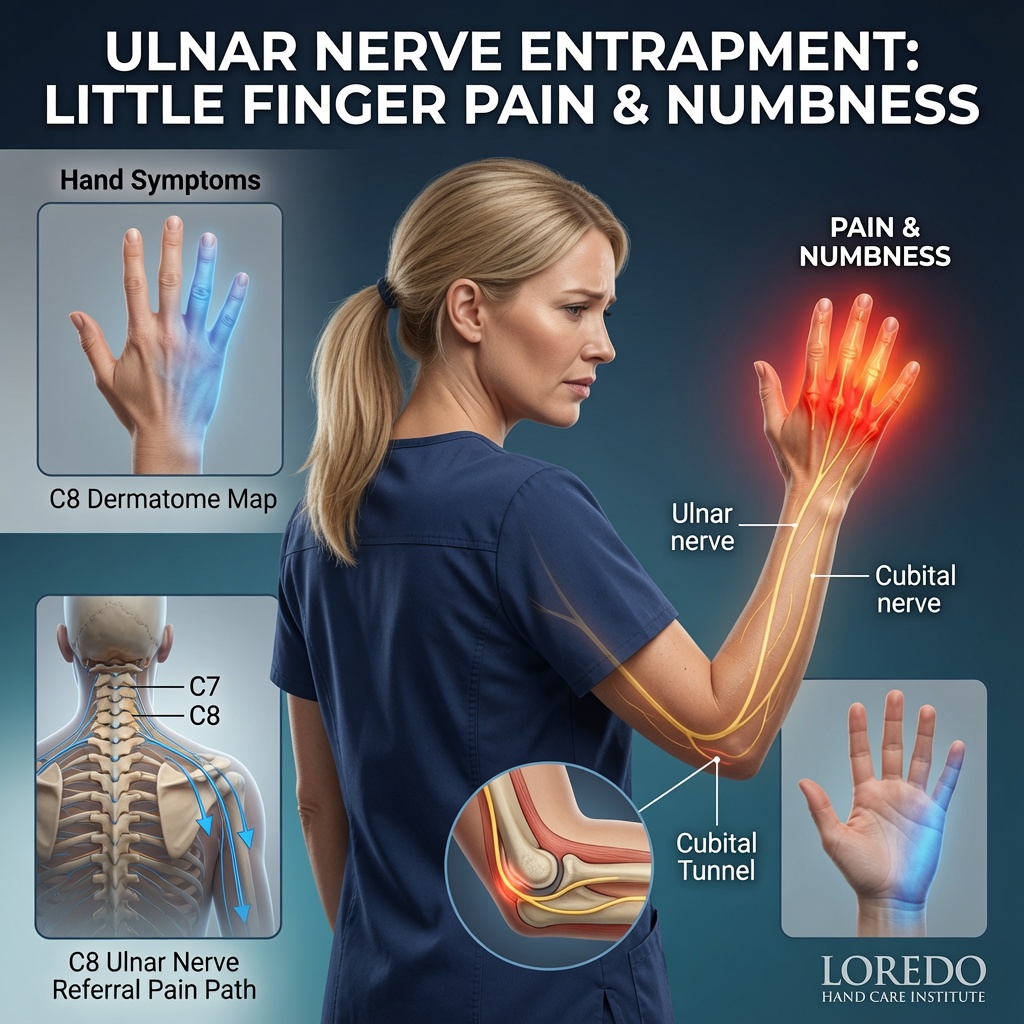
Golfer's elbow (medial epicondylitis) is the medial counterpart of tennis elbow, affecting the flexor-pronator tendon group at the inside of the elbow. Cubital tunnel syndrome compresses the ulnar nerve at the elbow and produces ring and small finger numbness. The two often coexist.
Volar (Palm-Side) Wrist Pain
Numbness, tingling, and night symptoms in the thumb-side fingers point to carpal tunnel syndrome. Tendon-specific pain on the radial wrist (FCR) or ulnar wrist (FCU) suggests wrist tendonitis. Aching forearm pain with median nerve symptoms that are not nocturnal suggests pronator teres syndrome.
Dorsal (Back-Side) Wrist Pain
A bump on the back of the wrist that fluctuates is most likely a ganglion cyst (see Hand Masses and Tumors). Tendon-specific pain in the six dorsal compartments is wrist tendonitis. Pain at the radial styloid that worsens with thumb motion is De Quervain's tendonitis.
Ulnar (Small-Finger Side) Wrist Pain
Pain on the ulnar side of the wrist that worsens with forearm rotation suggests a TFCC tear. Numbness in the ring and small fingers from a long bike ride or vibration tool work suggests Guyon's canal syndrome.
Thumb Base Pain
Deep aching pain at the base of the thumb that worsens with pinching, opening jars, or turning a key is most often thumb basilar joint arthritis (CMC arthritis). De Quervain's tendonitis sits slightly distal at the radial wrist and can be confused with CMC arthritis early on.
Palm Pain or Locking
A finger that catches or locks with bending suggests trigger finger. Progressive thickening and a finger that contracts toward the palm over months suggests Dupuytren's contracture. A new palm mass should be evaluated as a potential mass or tumor.
Finger and Knuckle Pain
Bony enlargements at the fingertip joints (Heberden's nodes) or the middle finger joints (Bouchard's nodes) point to hand and wrist arthritis. A drooping fingertip after a jam suggests mallet finger (see Extensor Tendon Injury). Symmetric inflammatory joint swelling at the MCP and PIP joints suggests rheumatoid arthritis.
Pain After Trauma
Persistent pain after a fall, blow, or twisting injury warrants imaging. Hand and finger fractures are common and should not be missed. Open lacerations with motion deficits suggest flexor or extensor tendon injury.
Pain by Symptom Pattern
What the pain feels like points to the underlying tissue type.
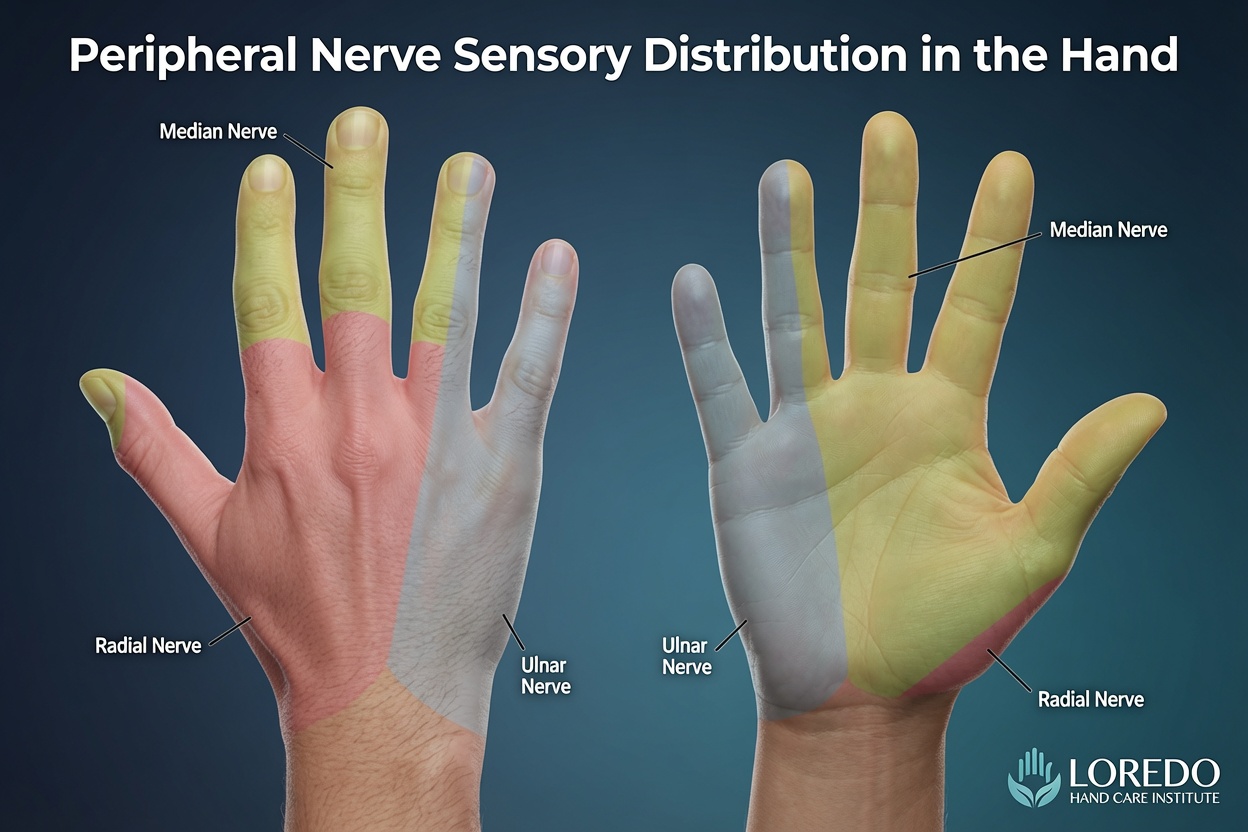
- Numbness or tingling in specific fingers nearly always means a nerve compression: carpal tunnel (thumb side), cubital tunnel or Guyon's (small finger side), or pronator teres (forearm pain plus median fingers).
- Locking, catching, or clicking of a finger means trigger finger.
- Pain that wakes you at night is classic for carpal tunnel (numbness pattern) and for severe rotator cuff or labral pathology of the shoulder (less likely for hand-specific issues).
- Pain with gripping and lifting usually means a tendon problem: tennis elbow (palm-down lifting), golfer's elbow (palm-up lifting), De Quervain's (thumb gripping), or wrist tendonitis.
- Deep aching joint pain with morning stiffness suggests arthritis. Less than 30 minutes of stiffness is more typical of osteoarthritis; more than 1 hour suggests rheumatoid arthritis.
- Finger color changes (white, blue, red) with cold or stress suggest Raynaud's disease.
- Constant pain at rest, particularly with a hard mass, is a red flag that warrants prompt evaluation.

Self-Care Before Your Visit
Most hand and elbow pain responds to simple measures while you wait for your appointment.
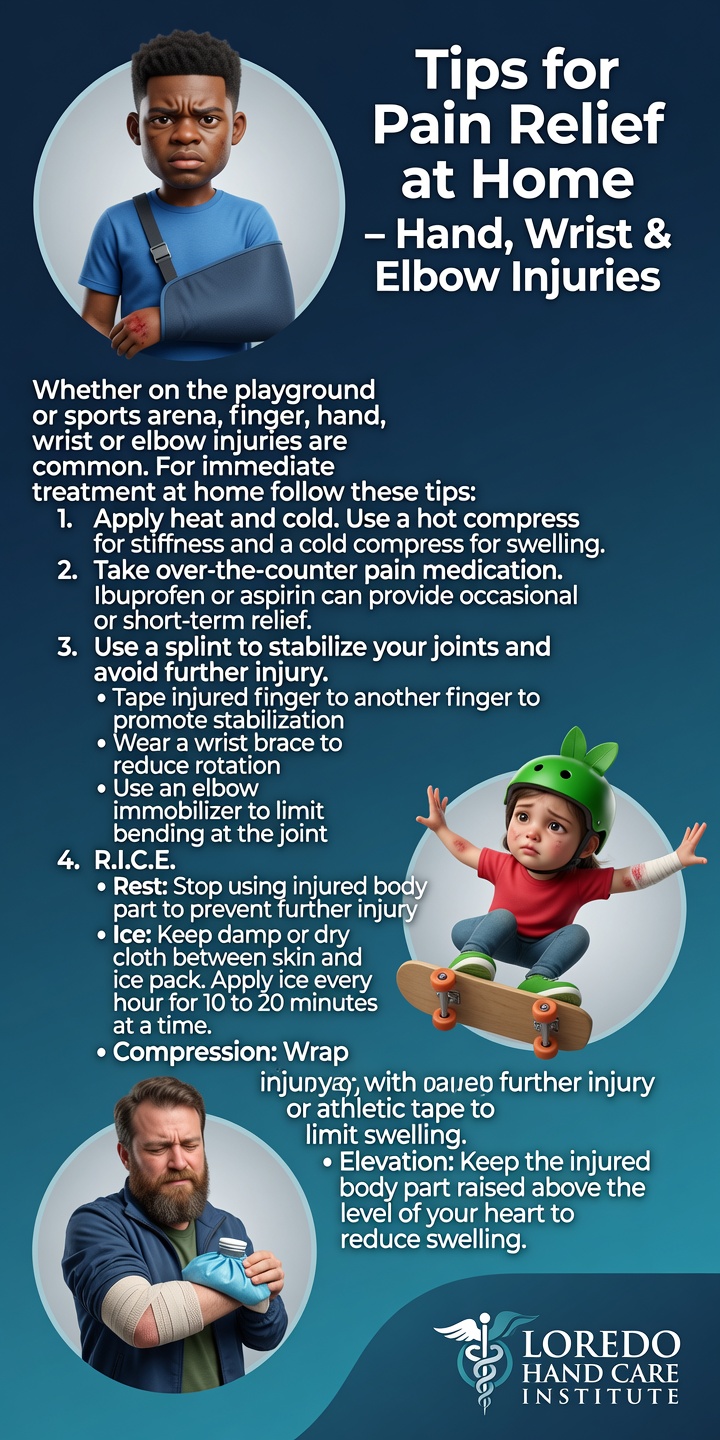
- Rest the affected area from the activity that aggravates symptoms.
- Ice 15 to 20 minutes several times a day for acute pain.
- Over-the-counter medication: ibuprofen, naproxen, or acetaminophen for symptom relief if you can take them safely.
- Splinting: drugstore wrist splints work well for suspected carpal tunnel symptoms (especially at night). Drugstore thumb spica splints help with De Quervain's. Buddy-tape an injured finger to its neighbor for stability.
- Activity modification: avoid the specific motion that produced symptoms.
- Document: note when symptoms started, what makes them worse and better, and what you have tried. Bring this to your visit.
- Bring prior imaging (X-rays, MRIs) on disc or via referring-physician portal if you have any.
When NOT to Wait: Emergency Red Flags
Call 911 or go directly to the nearest emergency department for any of the following:
- Open lacerations with active bleeding that does not stop with direct pressure
- Finger amputation (preserve the amputated part on ice in a clean bag, do not freeze it directly, and bring it with you)
- Fight bite wounds over the knuckle after a punch (high infection risk for septic arthritis)
- Severe crush injuries with deformity, exposed bone, or skin compromise
- Compartment syndrome signs: severe pain out of proportion to the injury, tense swelling, finger numbness or color change
- A pulseless, cold, or dusky finger (vascular compromise)
- Spreading redness or red streaks moving up the arm (suggests cellulitis or lymphangitis)
- High fever with a hand or arm wound (suspect deep infection or sepsis)
- Open fracture (bone visible through skin)
Call our office promptly (same day or next day) for any of these:
- Persistent pain after a fall that has not improved in 48 to 72 hours
- Sudden inability to bend or straighten a specific finger joint
- Concerning hand mass with red flag features (rapid growth, hard, fixed, painful at rest)
- New numbness or weakness that is constant rather than episodic
What to Expect at Your First Visit
A first visit at Loredo Hand Care Institute typically takes 30 to 60 minutes.
- Check-in and intake with the patient coordinator. Insurance is verified before your visit.
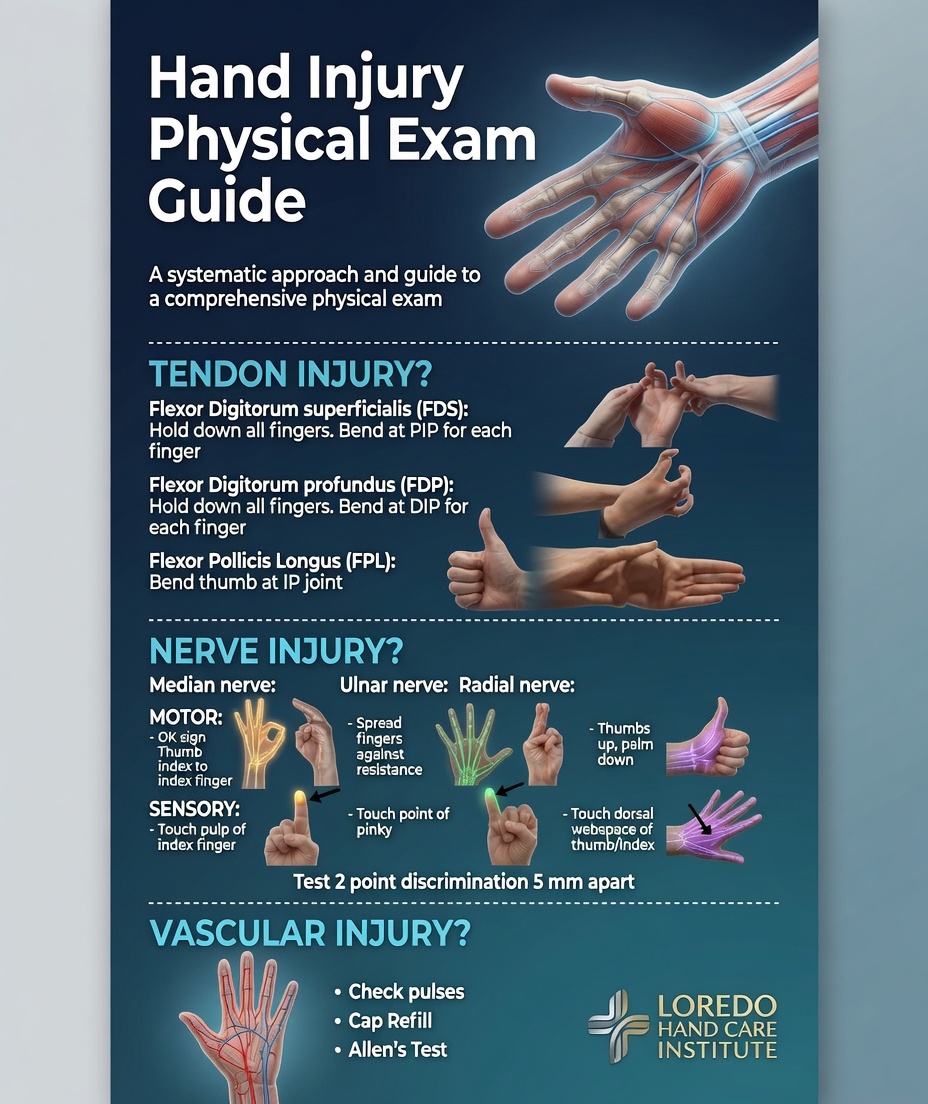
- History and examination with Dr. Loredo. He reviews your symptoms, asks about onset, mechanism, prior treatments, and performs a focused examination of the affected area. Provocative tests for nerve compression and tendon pathology are part of the standard exam.
- Imaging when appropriate. X-rays are obtained at the same visit when bone or joint pathology is suspected. Ultrasound and MRI are ordered when needed and scheduled at a convenient location.
- Working diagnosis and treatment plan. By the end of the visit, you will have a clear understanding of what is happening, what to do next, and what to expect.
- Treatment initiation. For most patients, conservative measures are started at the first visit (splinting, hand therapy referral, medication, in-office injection when indicated). Surgery, when appropriate, is usually scheduled within twenty-four to forty-eight hours of evaluation.
- Bilingual care. Spanish-speaking patients are welcomed and care is coordinated in Spanish at every step.
Frequently Asked Questions
When should I see a hand surgeon instead of my primary care doctor?
See a hand surgeon directly when you have hand or elbow symptoms that suggest a specific structural problem: numbness or tingling in specific fingers (suggests nerve compression), a locked or catching finger (suggests trigger finger), pain at a specific joint or tendon location, a visible mass or deformity, persistent pain after a fall or injury, or any symptoms that have not improved with rest and over-the-counter measures over 4 to 6 weeks. You do not need a referral from primary care for most insurance plans, and direct evaluation by a hand specialist often shortens the path to treatment. For non-specific aches, fatigue, or systemic joint pain, primary care or rheumatology evaluation is often a better first step.
Do I really need a specialist for this?
Many hand and elbow problems are simple enough that primary care, urgent care, or self-management is appropriate. The distinction is whether the symptom suggests a specific structural problem in the hand. Numbness, locking, catching, deformity, persistent post-injury pain, mass, and visible joint changes are signals for specialist evaluation. Generic aches, mild overuse pain, and non-specific joint discomfort are usually fine to manage with primary care first. When in doubt, calling our office for a brief phone triage is reasonable: our team can often tell you whether a hand surgeon visit is the right next step or whether another path is more appropriate.
What can I do at home before my visit?
Most hand and elbow pain responds to simple measures while you wait for your appointment. Rest the affected area from the activity that aggravates it. Ice 15 to 20 minutes several times a day for acute pain. Splint the affected wrist or finger if you have a splint at home (drugstore wrist splints work well for carpal tunnel and De Quervain's symptoms). Take over-the-counter NSAIDs (ibuprofen, naproxen) or acetaminophen for symptom relief if you can take them safely. Avoid the specific activity that produced symptoms. Bring a list of your symptoms, what you have tried, and any prior imaging or operative reports to your visit.
What does a first visit look like?
A first visit typically takes 30 to 60 minutes. Dr. Loredo reviews your history, asks about onset, mechanism, and pattern of symptoms, and performs a focused examination of the affected area. X-rays are obtained when bone or joint pathology is suspected, often at the same visit. Provocative tests for nerve compression and tendon pathology are performed in the exam room. At the end of the visit, you will have a working diagnosis, a treatment plan, and a clear sense of what to expect next. For most patients, conservative measures are started at the first visit. Surgery, when indicated, is usually scheduled within twenty-four to forty-eight hours of evaluation.
What symptoms mean I should not wait?
Open lacerations with bleeding, finger amputations, fight bites over the knuckle, deformities with skin compromise, severe crush injuries, signs of compartment syndrome (severe pain out of proportion plus tense swelling), and threatened tissue loss from infection or vascular compromise are emergencies that require 911 or emergency department care immediately. Severe pain after a fall, sudden inability to move a finger or thumb, fever with redness around a wound or joint, and rapidly expanding redness on the hand or arm warrant same-day evaluation. When in doubt about whether a symptom is urgent, call our office or go to an emergency department.
When to Call the Doctor
Call our office to schedule a visit if you experience any of the following:
- Hand or elbow pain that has lasted more than 4 to 6 weeks
- Numbness, tingling, or weakness in specific fingers
- A finger that catches, clicks, or locks
- A visible mass or lump on the hand, wrist, or fingers
- Pain after a fall, blow, or twisting injury that has not improved
- Joint deformity, contracture, or progressive loss of motion
- Failed conservative care from primary care
- Concerning hand symptoms in pregnancy or postpartum
- Workplace hand or upper extremity injury
For any medical emergency, call 911 or go to the nearest emergency department.
Related Conditions
- Carpal Tunnel Syndrome: median nerve compression at the wrist, the most common reason for hand surgery referral.
- Trigger Finger: catching or locking of a finger.
- Cubital Tunnel Syndrome: ulnar nerve compression at the elbow.
- Thumb Basilar Joint Arthritis: deep thumb base pain with pinching.
- De Quervain's Tendonitis: radial wrist pain with thumb motion.
- Tennis Elbow: lateral elbow pain with gripping.
- Golfer's Elbow: medial elbow pain with gripping.
- Hand and Finger Fractures: post-injury bone pain.
- Hand and Wrist Arthritis: chronic joint pain and morning stiffness.
- Hand Masses and Tumors: any new lump on the hand or wrist.
- Workers' Compensation Injuries: workplace hand injuries.
From the Blog
- Ergonomic Tips for Hand Pain at Work and Home: strategies by profession and tool selection.
- When a Cortisone Injection Is the Right Choice: which conditions respond and which do not.
- Why Same-Week Hand Surgery Matters: when waiting helps and when it does not.
Watch: Hand and elbow pain triage
Short videos from Dr. Loredo's Instagram and Facebook channels.